UPDATE August 4th, 2013. The CMS 2-Midnight rule is official. On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule [CMS-1599-F] updating fiscal year (FY) 2014 Medicare payment policies and rates under the Inpatient Prospective Payment System (IPPS) and the Long-Term Care Hospital Prospective Payment System (LTCH PPS). As part of this ruling the 2-Midnight rule was codified into law. The final rule modifies and clarifies CMS’s longstanding policy on how Medicare contractors review inpatient hospital admissions for payment purposes. Under this final rule, in addition to services designated as inpatient-only, surgical procedures, diagnostic tests and other treatments are generally appropriate for inpatient hospital admission and payment under Medicare Part A when the physician (1) expects the beneficiary to require a stay that crosses at least two midnights and (2) admits the beneficiary to the hospital based upon that expectation. This policy responds to both hospital calls for more guidance about when a beneficiary is appropriately treated—and paid by Medicare—as an inpatient, and beneficiaries’ concerns about increasingly long stays as outpatients due to hospitals’ uncertainties about payment.
The final rule specifies that the time frame used in determining the expectation of a stay surpassing two midnights begins when the beneficiary starts receiving services in the hospital. This includes outpatient observation services or services in an emergency department, operating room or other treatment area. While the final rule emphasizes that the time a beneficiary spends as an outpatient before the formal inpatient admission order is not inpatient time, the physician—and the Medicare review contractor—may consider this period when determining if it is reasonable and generally appropriate to expect the patient to stay in the hospital at least two midnights as part of an admission decision. Documentation in the medical record must support a reasonable expectation of the need for the beneficiary to require a medically necessary stay lasting at least two midnights. If the inpatient admission lasts fewer than two midnights due to an unforeseen circumstance this also must be clearly documented in the medical record. This new policy begins October 1st, 2013. You can read more about this major change at these links below. Additional commentary beyond these links represents my initial publication in May.
I tip my hat to all my fellow hospitalists who refuse to commit Medicare fraud in the interest of patient satisfaction. It just doesn't happen, ever. We are an honest breed. I know all my fellow brethren follow this wholesome practice style and have never even considered holding on to a patient just-one-more-day to qualify them for their three midnight stay in the hospital. And for that, we are going to be rewarded by Medicare. Hold on to your seats. Medicare just gave us a bombshell that promises to change how we practice medicine forever. They're calling it the 2-midnight rule (and 1-midnight rule too). The 2-midnight rule changes everything and we owe it to ourselves to get educated. We need to understand the importance of chart documentation requirements we will be asked to comply with starting October 1st, 2013. Read this whole article and then read it again and pass it on to all your hospitalist friends so they too can increase their value to hospitals. As hospital funding takes us on a race to the bottom, we must learn how to maximize our calorie intake at ObamaCare's Budget Buffet or we too will end up in the hospital as an observation admission for acute exacerbation of too-angry-for-discharge.
I have now been a hospitalist for ten years. A consistently frustrating job in my role as physician is my requirement to determine whether a patient should be admitted as inpatient or observation status. If you are a Medicare patient or a family member of a Medicare patient admitted to the hospital, you should always ask during your admission evaluation whether the order is being written for inpatient or observation. Don't ever assume that being admitted into the hospital means you are inpatient. If you have no idea what inpatient vs observation status means, you're not alone, but you owe it to yourself to understand. Medicare has an excellent patient resource to help explain all the important financial implications. I encourage all Medicare patients and their family to click this link and save the pdf file for quick review.
On April 26th, 2013, the Centers for Medicare & Medicaid Services (CMS) issued an assortment of proposed rule changes to update 2014 Medicare payment under the Inpatient Prospective Payment System (IPPS) to be applied to discharges on or after October 1st, 2013. Comments on these proposed rule changes will be accepted through June 25th, 2013 with a final ruling to be issued August 1st, 2013. The proposed rule change (CMS-1599-P, RIN 0938-AR53 ) was published in the Federal Registrar on May 10th, 2013. I have focused on the proposed rules changes detailed on pages 27644-27648 of the Federal Registrar document (page 160-164 of the pdf file). It's a fascinating look into the mind of Medicare madness. It has huge implications on how we practice medicine as a hospitalist and what we will be asked to document in the chart. It adds another layer of complexity to our role as documenteurs. This CMS fact sheet gives a summary of the proposed rules change. The bolded words are stressed by me.
As a result, many Medicare beneficiaries have experienced longer and more expensive stays in the hospital with higher Medicare Part B financial obligations during observation stays. Since 2006, the number of cases of Medicare beneficiaries experiencing greater than 48 hours of observation has increased from 3% in 2006 to 8% in 2011. This proposed rule is an attempt to help doctors and hospitals write inpatient orders, with a confidence that they will not be denied, if documentation continues to support physician expectations of greater than 2 days in the hospital providing medically reasonable and necessary care. Of course, even by their own admission, abuse potential is great and will be monitored. I have reviewed the proposed rule change, as it currently resides, on pages 27644-27648 of the registrar document. If you've gotten this far, you are obviously interested in this stuff so I encourage you to review it for yourself as well. It has a great potential to change how we practice and document as hospitalists for the simple fact that great hospitalists with additional fellowship training in documenting-smoke-and-mirrors can make anything look medically reasonable and necessary. The abuse potential they fear is going to hit Medicare financing straight in the noggin. Just look at the three midnight rule. Patients who are alive, but not really, get shipped off everyday to skilled nursing facilities after their 3-midnight hospital stay for acute exacerbation of frozen body syndrome because they can. Let's take a look at the proposed changes, shall we?
For the first time, as far as I can tell, CMS is telling hospitals and physicians that length of treatment will determine whether patients qualify for inpatient or observation status. The proposed rule is directing carriers to presume hospital inpatient admissions are reasonable and necessary if they cross two midnights and the hospital services are medically necessary and appropriate. Page 27644 of the Federal Registrar details the proposed rule change, with the following statement:
Policy Proposal on Admission and Medical Review Criteria for Hospital Inpatient Services under Medicare Part A

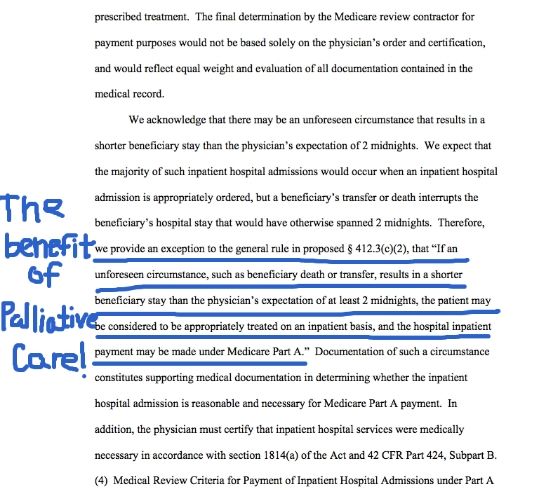
Before this proposed rule change, the only requirements for inpatient status were a physician (or other qualified practitioner) order and medical necessity. On page 27645 (bottom left paragraph) of this document, stakeholders recommended redefining the parameters to include a beneficiary's length of stay at the hospital. This section below is detailed from the bottom left to the top right of page 27645. Pay special attention to section between the blue arrows I have highlighted at the end:


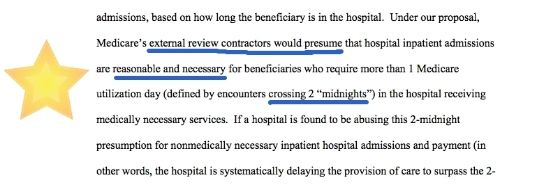
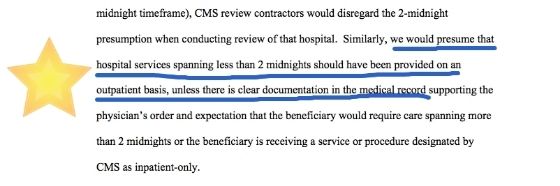
There you have it folks. For the first time, Medicare is going to define length of a hospital stay as reasonable and necessary based on how long patients are in the hospital or are even just expected to be in the hospital. How is this proposed rule change going to be applied in real life? Fast forward to bottom right paragraph on page 27645 to the top left of page 27646 and the proposed rules change gets even juicier. It describes how Medicare's external review contractors will be required to act:


I think this single paragraph on the proposed rule change is going to transform how hospitalists document in the chart. Medicare has defined for us exactly what is reasonable and necessary for inpatient care. The answer is two midnights. The way I see it, the 2-midnight rule is now our value mandate as a practicing specialty. We have been given the two-midnight rule and I guarantee to all that is true in this world, this is going to be the Bible for hospitalist medicine. Hospitalists that can document a yellow brick road straight to the top of Two Midnight Mountain are going to see their value to administrators explode as diagnosis related groups (DRGs) are the drug of choice for hospitals addicted to Medicare dollars.
External review contractors are now required to presume the threshold of reasonable and necessary for 2-midnight stays. Experienced hospitalists have an amazing ability to provide documentation supporting medically necessary care to anything that barely breaths, barely moves or barely speaks in our chronically alive, but not really patients admitted for medically necessary and reasonable nursing home care. Everything great hospitalists do is medically necessary because their documentation says so. Great hospitalists are worth their weight in gold for this very reason. External review contractors will never be able to show abuse of the 2-midnight presumption by hospitalist groups with great documentations skills. This. Is What. Hospitalists. Do. For. A. Living. Hospitalists are documentation experts. They play that game better than anyone. Hospital systems aren't going to subsidize hospitalists $140,000 per year per hospitalist for nothing. For all intents and purposes, hospitalists are documentation whores and hospitals are their pimps.
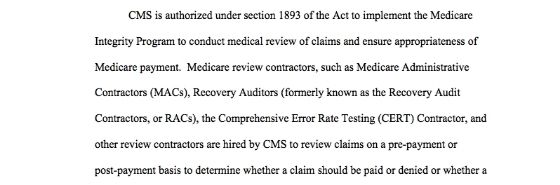
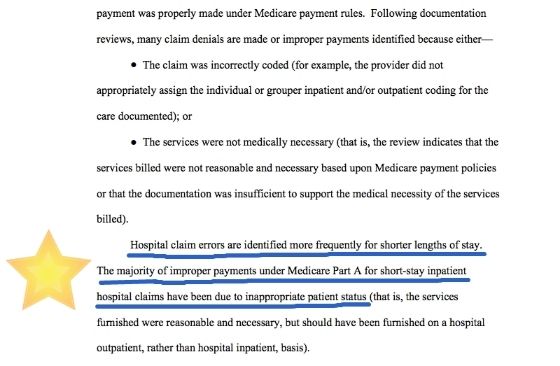
How do hospital inpatient payments currently get denied? The middle left column of page 27647 to top middle column of the same page provides a nice summary detailed below. In a nutshell, payments made in error by CMS are more frequently associated with short stay procedural inpatient claims that should have been provided on a hospital outpatient basis, which I believe is the driving force behind this proposed rule change:


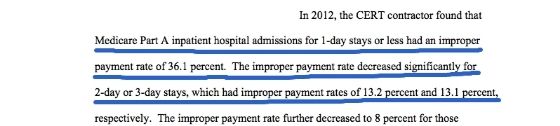
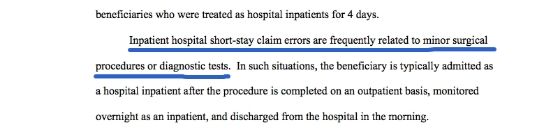
How bad have the errors been? Continuing on with the middle column on page 27647:


In Medicare's eyes, the errors are due to procedures, not little old grandpa admitted with acute exacerbation of too-unsteady-to-ballroom-dance and have nothing to do with hospitalist patients who also get three inpatient midnights for a primary diagnosis of too-wrinkled-to-smile. As a hospitalist, I am not admitting observation patients who just had an EGD or heart catheterization. I am admitting my 98 year old grandmothers who's family can't take care of them anymore so they drop them off at the emergency room for us to handle instead of placing them in a nursing home because they refuse to sell off her assets to qualify for Medicaid instead of planning for the future and purchasing long term care insurance policies.
"Did you know 'to angry for discharge' and 'patient refuses to leave the ER' are now Medicare approved reasons for inpatient admission?"


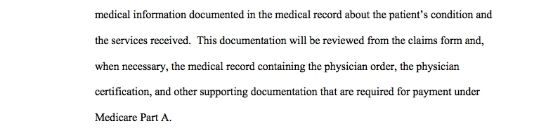
These are patients where hospitalists with exceptional documentation skills can make anything medically reasonable and necessary and show value under the 2-midnight rule where no value previously existed. This documentation is important because Medicare clearly says part way down from the top right column on page 27647 that a physician order for inpatient shall not by itself make a patient qualified. The medical necessity review rule continues as follows:


In other words, just because the physician writes an order for inpatient, it doesn't mean the inpatient status is automatically correct. This gets me back to my original issue. If the physician order isn't the law, then why have the requirement in the first place. Why not bypass the physician and have a process in place that allows people trained in the determination of inpatient vs outpatient make the determination. Why not allow hospital utilization review experts to make determinations on a retrospective basis and get rid of all the errors we have to deal with under this process. I would love to write an order for "Hospital bed: status per utilization review team" and have Medicare pay for all charges up to that moment in time regardless of the status of the patient. That would make patients happy.
In addition to the physician order, medical necessity reviews will continue as described in the medical review criteria for all hospital services and the inpatient hospital admission guidelines. The first paragraph at the top of page 27648 starts this discussion below. I believe this entire page is vitally important and every hospitalist should read them and learn them. The rules detailed on this page are going to transform how we document our social admits who are too-old-to-breath-in-the-upright-position so they can get qualified for three midnights under a diagnosis of need-two-on-the-way-to-three-midnightitis :




It's all about documentation people. Clear as day, Medicare is going to focus on patients who are being billed inpatient who do not stay more than 2 midnights. They may continue to audit the rest, but they are not going to focus their energies on that population unless they find an attempt to game the system (as if somehow the 3-midnight SNF rule is not being gamed). Great hospitalists could get any patient who is admitted with a diagnosis of patient-becomes-invisible-due-to malnutrition-and-old-age-when-they-turn-sideways-but-they-have-no-other-medical-problems qualified for a ten day hospital stay with reasonable and necessary medical care. I hate to tell Medicare the bad news, but from where I'm sitting in the peanut gallery, the entire country is gaming the Medicare system. It's-All-One-Giant-Game. The 3 midnight rule is already a farce. We now have the 2-midnight rule too! Hurray! Oh, and the 1-midnight-rule too! Yeah!
Medicare's rule change has just given hospitalists the social admit green light to write inpatient orders on all their patients with acute exacerbations of too-demented-to-care-about-paying-for-a-nursing-home-but-the-daughter-wants-the-farmland. Why do I say this? Because Medicare clearly states they are going to use physician documentation of the "reasonable basis for the expectation of a stay crossing 2-midnights" that will justify the medical necessity of the inpatient admission. If this isn't an entry into the Inpatient Social Admit Marathon, then you're not reading what I'm reading. Social admits ALWAYS take longer than two midnights to disposition out of the hospital. If a hospitalist states on admission that they think their admission for too-slothy-to-support-themselves is going to be in the hospital longer than two midnights, all they need to do is document their supporting reasons. They state that clear as day:
"Ask your hospitalist today if mom is too old to hyperventilate and they'll work the system to get her a free entry into the Nursing Home Marathon paid for by Medicare."

Every social admit a hospitalist is asked to admit into the hospital could qualify for inpatient based on the expectation of the process taking longer than two midnights to provide an appropriate discharge to the community (especially at really crappy hospitals) and documenting their judgement of risk for an adverse event if they are not discharged to a nursing facility. They way I see it, Medicare is telling me I can qualify my 98 year old patient who is too-weak-to-hyperventilate as inpatient status by simply writing the following statement:
Just wait until the general public gets a hold of this change. No longer do they need to worry about caring for grandma at home. Just bring them to the adult humane society (aka the ER), get them their two midnights on the way to the mandatory three SNF midnights and it's a Friday night SNF party at the fancy nursing home with skilled nurses. Once hospitalists get past that second midnight with inpatient status while ruling out occult bacteremia in the absence of fever, absence of leukocytosis and the absence of standard of care, they can easily get their third SNF midnight by documenting their need to confirm acute exacerbation of needs-three-midnights-and-a-place-to-live-upon-discharge.
Alternatively, I'm fascinated by all the acute drug overdose patients who require ventilator support in the ICU that are admitted at 1 am and are discharged by 3 pm. Apparently, they aren't in the hospital long enough to be admitted inpatient if the hospitalist believes they can be discharged before the following night. Apparently, they are only being observed on the ventilator to determine whether or not to actually turn the ventilator on. Being sick on the ventilator for less than one midnight just doesn't cut it anymore. If you want to qualify your critically ill drug overdose for inpatient, you'd best consider telling the family to go home and get more drugs to double the suicide dose so the hospitalist doesn't extubate them too soon from life support. It's a matter of life or 2-midnights.
However, If hospitalists document their confidence in their excellent care team and can get their critically ill patient discharged in less than two midnights, their hospital may be punished. They should instead consider providing suboptimal care, generate an iatrogenic critical medication error or two and delay the discharge past the second midnight to verify payment under inpatient status. Or maybe they should just delay their discharge for another midnight so their clearly obvious inpatient care gets paid for as an inpatient and not the less funded observation rate.
Yes folks, Medicare gave hospitalists the 3-midnight rule. Now they are preparing to give hospitalists the 2-midnight and 1-midnight rules. On October 1st, 2013, how hospitalists document their social admits will provide a great opportunity for them to show value where none previously existed. Turn that observation frown upside down and give your 108 year old with a mild case of too-old-to-calculate-her-age-based-on-her-date-of-birth a golden ticket to inpatient status and one small midnight away from the dream SNF of her choice. You owe it to her. She's 108 years old and you're not.
Some of this post is for entertainment purposes only and likely contains humor only understood by those in a healthcare profession. Read at your own risk. Including the hundreds of original Happy Hospitalist crude medical ecards on Pinterest.
Tweet
The final rule specifies that the time frame used in determining the expectation of a stay surpassing two midnights begins when the beneficiary starts receiving services in the hospital. This includes outpatient observation services or services in an emergency department, operating room or other treatment area. While the final rule emphasizes that the time a beneficiary spends as an outpatient before the formal inpatient admission order is not inpatient time, the physician—and the Medicare review contractor—may consider this period when determining if it is reasonable and generally appropriate to expect the patient to stay in the hospital at least two midnights as part of an admission decision. Documentation in the medical record must support a reasonable expectation of the need for the beneficiary to require a medically necessary stay lasting at least two midnights. If the inpatient admission lasts fewer than two midnights due to an unforeseen circumstance this also must be clearly documented in the medical record. This new policy begins October 1st, 2013. You can read more about this major change at these links below. Additional commentary beyond these links represents my initial publication in May.
- Fact sheet
- More CMS information on the 2-midnight rule.
- Federal registrar. This is a very long document. You can find the general section on the 2 midnight rule by clicking on the link provided . Then search the document for "2-midnight". This can be done by hitting Control F (Command F on an Apple keyboard) and typing "2 midnight". This will take you to the area of discussion about the 2-midnight rule.
- FAQ PDF FILE (New as of October 1st, 2013). The first question explains the last minute enforcement delay that directs RAC auditors not to question any inpatient admission stay of one midnight or less for the first 90 days following October 1st, 2013
- "CMS will instruct the Medicare Administrative Contractors (MACs) and Recovery Auditors that they are not to review claims spanning more than two midnights after admission for a determination of whether the inpatient hospital admission and patient status was appropriate. In addition, for a period of 90 days, CMS will not permit Recovery Auditors to review inpatient admissions of one midnight or less that begin on or after October 1, 2013.
- On August 15th, 2013, CMS held a special lecture style open door forum discussion on the new rules. A transcript was released on August 22nd and is available for download this link here.
- September 5th, 2013. Hospital Inpatient Order And Certification.
- September 26th, 2013. Second Special Open Door Forum transcript.
- October 23, 2013: Here is the link to MLN SE1333 titled Temporary Instructions for Implementation of Final Rule 1599-F for Part A to Part B Billing of Denied Hospital Inpatient Claims.
- November 4th, 2013. Selecting Hospital Claims for Patient Status Reviews: Admissions On or After October 1, 2013. A CMS document.
- November 14th, 2013. The delay in enforcement by Recovery Auditors has been extended to March 31st, 2014. Here is the link with that information and other important FAQs. This has now been extended to September 30th, 2014 according to CMS.
- UPDATE November 27th, 2013. Reviewing Hospital Claims for Patient Status: Admissions On or After October 1, 2013. A CMS document.
- December 6th, 2013. More information on Inpatient Hospital Reviews from the CMS website.
- December 19th, 2013: Special Open Door Forum discussion information. This is the third forum discussion.
- MLN Matters SE1403: Probe & Educate Medical Review Strategy: Probe Reviews of Inpatient Hospital Claims and Corresponding Provider Outreach and Education.
- Occurrence Span Code 72; Identification of Outpatient Time Associated with an Inpatient Hospital Admission and Inpatient Claim for Payment
- Special Open Door Forum February 4th, 2014 1-2 PM ET. Conference call only. Participant Dial-In Number(s): (877) 251-0301; Conference ID # 47736519. Here's the link to the Open Door Forum CMS page with links to prior conference calls.
- MM8445 February 7th, 2014: Implementing the Part B Inpatient Payment Policies from CMS-1599F.
- January 30th, 2014: Hospital Inpatient Admission Order and Certification additional clarification.
- February 27th, 2014 MLN Connects National Provider Call 2:30-4:00 PM ET: 2-Midnight Benchmark: Discussion of the Hospital Inpatient Admission Order and Certification — Space is limited. Register here.
- Additional information relating to the order and certification provisions is located on the Hospital Center web page.
- Feedback and questions on the two midnight provision for admission and medical review can be sent to IPPSAdmissions@cms.hhs.gov
- MM8666 March 21st, 2014: Implementing the Part B Inpatient Payment Policies from CMS - 1599 - F;
- The SGR Patch (HR 4302) that was signed into law in Early April 2014 delays RAC enforcement of the 2-midnight rule until March 31st, 2015 and allows CMS to continue their "probe and educate" program until that time.
I tip my hat to all my fellow hospitalists who refuse to commit Medicare fraud in the interest of patient satisfaction. It just doesn't happen, ever. We are an honest breed. I know all my fellow brethren follow this wholesome practice style and have never even considered holding on to a patient just-one-more-day to qualify them for their three midnight stay in the hospital. And for that, we are going to be rewarded by Medicare. Hold on to your seats. Medicare just gave us a bombshell that promises to change how we practice medicine forever. They're calling it the 2-midnight rule (and 1-midnight rule too). The 2-midnight rule changes everything and we owe it to ourselves to get educated. We need to understand the importance of chart documentation requirements we will be asked to comply with starting October 1st, 2013. Read this whole article and then read it again and pass it on to all your hospitalist friends so they too can increase their value to hospitals. As hospital funding takes us on a race to the bottom, we must learn how to maximize our calorie intake at ObamaCare's Budget Buffet or we too will end up in the hospital as an observation admission for acute exacerbation of too-angry-for-discharge.
I have now been a hospitalist for ten years. A consistently frustrating job in my role as physician is my requirement to determine whether a patient should be admitted as inpatient or observation status. If you are a Medicare patient or a family member of a Medicare patient admitted to the hospital, you should always ask during your admission evaluation whether the order is being written for inpatient or observation. Don't ever assume that being admitted into the hospital means you are inpatient. If you have no idea what inpatient vs observation status means, you're not alone, but you owe it to yourself to understand. Medicare has an excellent patient resource to help explain all the important financial implications. I encourage all Medicare patients and their family to click this link and save the pdf file for quick review.
Medicare Part A rules apply if the physician writes an order for inpatient but Medicare Part B rules apply if the physician writes an order for observation. Observation is considered outpatient. That means all the copays, deductibles and coverage inclusions or exclusions are determined by what order the physician has written. Patients without supplemental insurance will get a bill for 20% of all charges incurred during an observation hospital stay because Medicare Part B only covers 80% of allowed outpatient Medicare charges. Patients without Medicare Part B will get a bill for full price. This mostly affects veterans who have Medicare Part A coverage but choose not to pay for Medicare Part B coverage due to their VA benefits. Most of these folks say they want to stay in their local hospital because they say, "I have Medicare". Most have no idea that not paying for Medicare Part B means they aren't covered for observation stays at their local hospital unless the VA is willing to pay for that care. I wouldn't count on that.
Most patients pay for Medicare Part B. Most patients have a supplemental policy too, so the issue is a non issue, except for payment of home medications administered in the hospital. The biggest problem occurs when physicians write an order for observation status and don't tell patients their routine self administered home medications will not be paid for by their Medicare insurance if the hospital provides these pills for them. Patients also have an obligation to educate themselves about the rules of their plan. Because Medicare will not pay, neither will a patient's supplemental policy. That means the hospital will send their patient a very large bill for the $25 dollar Tylenol given for their observation stay for headache, thus causing them another trip to the ER and observation admission for chest pain when they get their $2,000 bill three weeks after discharge. Since this $25 Tylenol is not covered under insurance, the patient gets no benefit of the insurance discount. In addition, I would not always count on Medicare Part D picking up the tab. They may, under certain circumstances, but I wouldn't consider that option reliable. Grandma gets to pay full price for that $25 pain pill. Oops, sorry about that, right?
I have a personal rule to notify every patient I admit observation status into the hospital of this hole in their Medicare coverage so I can give them the opportunity to either provide their home medications for my hospital to verify and administer by the nurse or to hold all their routine home medications until their expected less than 48 hour observation stay has been completed. Sometimes doctors may even look the other way while recommending patients take their own pills without telling anyone. Universally, patients are grateful for my discussion. Unfortunately, this uncompensated time isn't paid for and doesn't affect patient satisfaction scores. That only applies to inpatients. It is a freebie for my time out of respect for my patient's sanity. Unfortunately, I am the exception to the rule. Nobody explains this rule to patients so they can understand the implications to their financial health. I have stopped counting how many times I have heard angry patients describe their bills for several thousand dollars they received three weeks after a 24 hour stay in the hospital. It's a good thing their anger doesn't count for patient satisfaction scores. Maybe that's why nobody takes the time to care.
Determining inpatient or observation status is complex. Medicare says physicians must write an inpatient order for hospitals to get paid for inpatient care (Medicare Part A rules), but having a physician write the order does not guarantee Medicare will pay. Medicare wants it both ways. They require the order but refuse to accept the order as law. So my question becomes, why require a physician order if the order has no teeth? Why not develop a different process that provides experts with the opportunity make the decision. I have no idea why physician input is even relevent. Physicians aren't trained to know this stuff. We are guessing 100% of the time. That's right folks, physicians are not trained to know all the details required for Medicare to pay or deny an inpatient stay. So we guess, every time. All of us. It's irrational, I know. Most hospitals have utilization review experts that scour the patient chart for information to determine whether my order for inpatient or observation status was correct, but this rarely happens in real time. If I get it right, nothing happens. If I get it wrong, I am often asked to consider writing an order to change the status, which may affect patient coverage for self administered medications already provided. Oops, sorry about that, right? It's a shameful way to treat patients.
What are physicians thinking about on admission? In addition to evaluation and stabilization, the medical plan from the start often revolves around methods to quickly and safely get the patient discharged to the next appropriate level of care. That may mean physicians provide an intensity of service much higher than would be expected for the patient's number-of-wrinkles/age ratio. That may mean an aggressively documented thought process to include one-in-a-million-doc types of conditions that would make any residency director put on their pimping caps with an excitement only a morning report can provide. This process defines skilled nursing facility (SNF) driven medicine all across this country. EMTALA is the leaky faucet and "sniffs" are the plumber. The moment patients are admitted to a hospital, the astute hospitalist is already formulating a plan to get free front row tickets in the too-weak-to-pee-on-my-own section of the the three-midnight-road-rally paid for by the Medicare National Bank.
Hospitalists are writing orders and aggressively documenting their grave concerns about acute exacerbation of too-old-to-answer-a-question-without-telling-a-story as a reason to meet inpatient criteria and writing essays about why inpatient status is required to qualify for a three midnight hospitel stay and early disposition to the land of skilled nurses in a nursing home. It happens everywhere in this country, except on my service and in my hospital. Trust me. I refuse to play that atrocious game. My patients whom I admit with acute exacerbation of too-old-to-go-home and life threatening cases of upset-son-is-demanding-admission only get exactly what they need and not a thing more. They don't get medically reasonable and necessary intravenous fluids running at 150 cc/hour for 72 hours because their baseline creatinine is 1.223. They do not get medically reasonable and necessary every 4 hour neuro checks for 72 hours because they're pinky toe is numb without explanation after being stepped on by a farm animal. They won't get that MRI on day three, making sure to wait until agressive hydration has been achieved and they definitely won't get the blood cultures that require inpatient monitoring to rule out sepsis as a contribution to their three year battle with perma-supine syndrome. No. Sir. Ree. My patients don't get any of that medically reasonable and necessary care to get them qualified for their three midnight stay and a golden ticket to the palace in the Sniffdom of their choice provided for under medically reasonable and necessary Medicare benefits paid for by IOUs to the Canadian, British and Chinese governments.
Are you confused yet? Well, things are about to change, again. Many Medicare carriers determine appropriateness of inpatient status by using a combination of diagnosis and intensity of service to determine whether inpatient criteria has been met. For example, diagnoses such as back pain, chest pain, pain in my ass, weakness, syncope and abdominal pain won't get you qualified for inpatient status unless you have a really good hospitalist with extra fellowship training treating exacerbation of needthreemidnightitis as a Medicare approved major complication and comorbidity. When I write the wrong order, lots of paper work must happen for the hospital to get paid. Even I have to retroactively change my billing to match the hospital status or my physician claims will get denied. Most doctors aren't trained on any of this stuff.
What are physicians thinking about on admission? In addition to evaluation and stabilization, the medical plan from the start often revolves around methods to quickly and safely get the patient discharged to the next appropriate level of care. That may mean physicians provide an intensity of service much higher than would be expected for the patient's number-of-wrinkles/age ratio. That may mean an aggressively documented thought process to include one-in-a-million-doc types of conditions that would make any residency director put on their pimping caps with an excitement only a morning report can provide. This process defines skilled nursing facility (SNF) driven medicine all across this country. EMTALA is the leaky faucet and "sniffs" are the plumber. The moment patients are admitted to a hospital, the astute hospitalist is already formulating a plan to get free front row tickets in the too-weak-to-pee-on-my-own section of the the three-midnight-road-rally paid for by the Medicare National Bank.
Hospitalists are writing orders and aggressively documenting their grave concerns about acute exacerbation of too-old-to-answer-a-question-without-telling-a-story as a reason to meet inpatient criteria and writing essays about why inpatient status is required to qualify for a three midnight hospitel stay and early disposition to the land of skilled nurses in a nursing home. It happens everywhere in this country, except on my service and in my hospital. Trust me. I refuse to play that atrocious game. My patients whom I admit with acute exacerbation of too-old-to-go-home and life threatening cases of upset-son-is-demanding-admission only get exactly what they need and not a thing more. They don't get medically reasonable and necessary intravenous fluids running at 150 cc/hour for 72 hours because their baseline creatinine is 1.223. They do not get medically reasonable and necessary every 4 hour neuro checks for 72 hours because they're pinky toe is numb without explanation after being stepped on by a farm animal. They won't get that MRI on day three, making sure to wait until agressive hydration has been achieved and they definitely won't get the blood cultures that require inpatient monitoring to rule out sepsis as a contribution to their three year battle with perma-supine syndrome. No. Sir. Ree. My patients don't get any of that medically reasonable and necessary care to get them qualified for their three midnight stay and a golden ticket to the palace in the Sniffdom of their choice provided for under medically reasonable and necessary Medicare benefits paid for by IOUs to the Canadian, British and Chinese governments.
Are you confused yet? Well, things are about to change, again. Many Medicare carriers determine appropriateness of inpatient status by using a combination of diagnosis and intensity of service to determine whether inpatient criteria has been met. For example, diagnoses such as back pain, chest pain, pain in my ass, weakness, syncope and abdominal pain won't get you qualified for inpatient status unless you have a really good hospitalist with extra fellowship training treating exacerbation of needthreemidnightitis as a Medicare approved major complication and comorbidity. When I write the wrong order, lots of paper work must happen for the hospital to get paid. Even I have to retroactively change my billing to match the hospital status or my physician claims will get denied. Most doctors aren't trained on any of this stuff.
UPDATED May 31st, 2013 with new page references to the appropriate files detailed below. The original source file is no longer active.
On April 26th, 2013, the Centers for Medicare & Medicaid Services (CMS) issued an assortment of proposed rule changes to update 2014 Medicare payment under the Inpatient Prospective Payment System (IPPS) to be applied to discharges on or after October 1st, 2013. Comments on these proposed rule changes will be accepted through June 25th, 2013 with a final ruling to be issued August 1st, 2013. The proposed rule change (CMS-1599-P, RIN 0938-AR53 ) was published in the Federal Registrar on May 10th, 2013. I have focused on the proposed rules changes detailed on pages 27644-27648 of the Federal Registrar document (page 160-164 of the pdf file). It's a fascinating look into the mind of Medicare madness. It has huge implications on how we practice medicine as a hospitalist and what we will be asked to document in the chart. It adds another layer of complexity to our role as documenteurs. This CMS fact sheet gives a summary of the proposed rules change. The bolded words are stressed by me.
Admission and Medical Review Criteria for Inpatient Services.
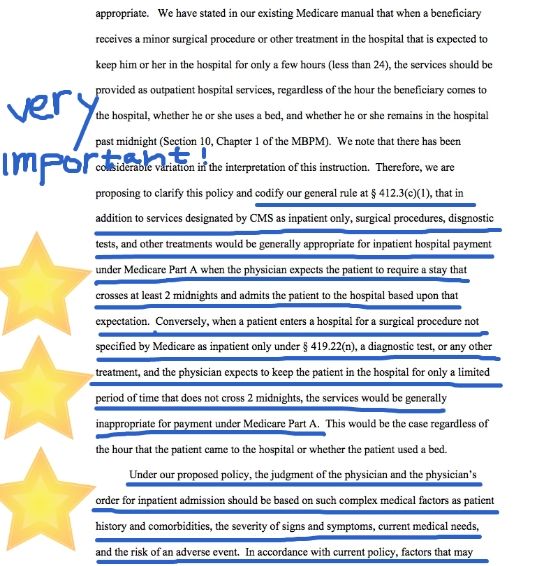
In the proposed rule, CMS clarifies its longstanding policy on how Medicare contractors review inpatient admissions for payment purposes. Under this proposed rule, CMS is proposing that hospital inpatient admissions spanning at least two midnights (that is, at least more than one Medicare utilization day), will presumptively qualify as appropriate for payment under Medicare Part A. Conversely, hospital inpatient admissions spanning less than two midnights (that is, less than one Medicare utilization day) will presumptively be inappropriate for payment under Medicare Part A.
This presumption may be overcome by documentation in the medical record supporting the admitting physician’s expectation that the beneficiary would need care spanning at least two midnights and an unforeseen circumstance results in a shorter beneficiary stay than the physician’s expectation. Physicians must support their expectation, and accordingly their order for admission, through clear and complete medical documentation. This proposed policy would address longstanding concerns from hospitals that they need more guidance on when a patient is appropriately treated and paid by Medicare as an inpatient. At the same time the proposed change would help beneficiaries who in recent years have been having longer stays as outpatients because of hospital uncertainties about payment if they admit the patient to the hospital.Let me give you a little background about why Medicare is making some changes. Medicare is bankrupt. As a result, they have a program in place to retroactively take back money paid to hospitals for services they may determine not to be medically necessary and appropriate. Much of the recovery has focused on inpatient hospital stays of short duration. Hospitals responded by approaching physicians with recommendations to admit patients as observation status instead of inpatient status or apply observation status to patients already admitted as inpatient in an effort to avoid denial of payment from Medicare. Hospitals want to get paid. Medicare doesn't want to pay. Do you see the problem here?
As a result, many Medicare beneficiaries have experienced longer and more expensive stays in the hospital with higher Medicare Part B financial obligations during observation stays. Since 2006, the number of cases of Medicare beneficiaries experiencing greater than 48 hours of observation has increased from 3% in 2006 to 8% in 2011. This proposed rule is an attempt to help doctors and hospitals write inpatient orders, with a confidence that they will not be denied, if documentation continues to support physician expectations of greater than 2 days in the hospital providing medically reasonable and necessary care. Of course, even by their own admission, abuse potential is great and will be monitored. I have reviewed the proposed rule change, as it currently resides, on pages 27644-27648 of the registrar document. If you've gotten this far, you are obviously interested in this stuff so I encourage you to review it for yourself as well. It has a great potential to change how we practice and document as hospitalists for the simple fact that great hospitalists with additional fellowship training in documenting-smoke-and-mirrors can make anything look medically reasonable and necessary. The abuse potential they fear is going to hit Medicare financing straight in the noggin. Just look at the three midnight rule. Patients who are alive, but not really, get shipped off everyday to skilled nursing facilities after their 3-midnight hospital stay for acute exacerbation of frozen body syndrome because they can. Let's take a look at the proposed changes, shall we?
For the first time, as far as I can tell, CMS is telling hospitals and physicians that length of treatment will determine whether patients qualify for inpatient or observation status. The proposed rule is directing carriers to presume hospital inpatient admissions are reasonable and necessary if they cross two midnights and the hospital services are medically necessary and appropriate. Page 27644 of the Federal Registrar details the proposed rule change, with the following statement:
Policy Proposal on Admission and Medical Review Criteria for Hospital Inpatient Services under Medicare Part A

External review contractors are now required to presume the threshold of reasonable and necessary for 2-midnight stays. Experienced hospitalists have an amazing ability to provide documentation supporting medically necessary care to anything that barely breaths, barely moves or barely speaks in our chronically alive, but not really patients admitted for medically necessary and reasonable nursing home care. Everything great hospitalists do is medically necessary because their documentation says so. Great hospitalists are worth their weight in gold for this very reason. External review contractors will never be able to show abuse of the 2-midnight presumption by hospitalist groups with great documentations skills. This. Is What. Hospitalists. Do. For. A. Living. Hospitalists are documentation experts. They play that game better than anyone. Hospital systems aren't going to subsidize hospitalists $140,000 per year per hospitalist for nothing. For all intents and purposes, hospitalists are documentation whores and hospitals are their pimps.
How do hospital inpatient payments currently get denied? The middle left column of page 27647 to top middle column of the same page provides a nice summary detailed below. In a nutshell, payments made in error by CMS are more frequently associated with short stay procedural inpatient claims that should have been provided on a hospital outpatient basis, which I believe is the driving force behind this proposed rule change:
"Did you know 'to angry for discharge' and 'patient refuses to leave the ER' are now Medicare approved reasons for inpatient admission?"

These are patients where hospitalists with exceptional documentation skills can make anything medically reasonable and necessary and show value under the 2-midnight rule where no value previously existed. This documentation is important because Medicare clearly says part way down from the top right column on page 27647 that a physician order for inpatient shall not by itself make a patient qualified. The medical necessity review rule continues as follows:
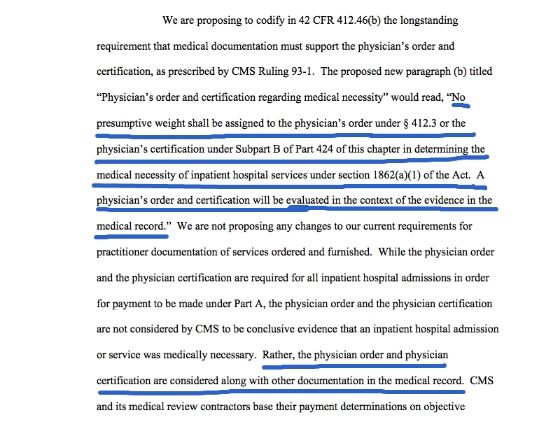
In addition to the physician order, medical necessity reviews will continue as described in the medical review criteria for all hospital services and the inpatient hospital admission guidelines. The first paragraph at the top of page 27648 starts this discussion below. I believe this entire page is vitally important and every hospitalist should read them and learn them. The rules detailed on this page are going to transform how we document our social admits who are too-old-to-breath-in-the-upright-position so they can get qualified for three midnights under a diagnosis of need-two-on-the-way-to-three-midnightitis :

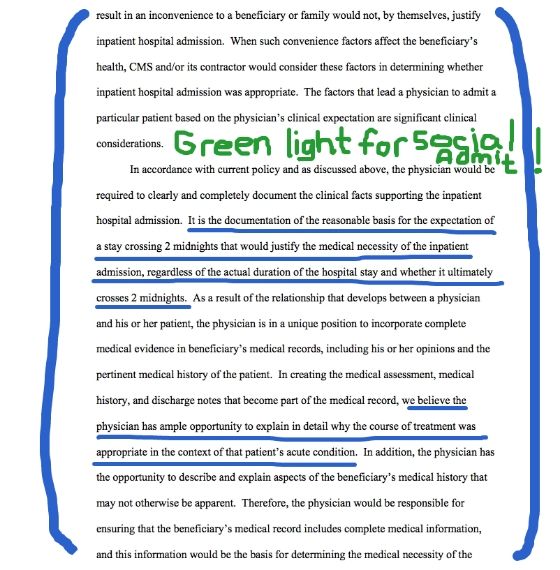
Medicare's rule change has just given hospitalists the social admit green light to write inpatient orders on all their patients with acute exacerbations of too-demented-to-care-about-paying-for-a-nursing-home-but-the-daughter-wants-the-farmland. Why do I say this? Because Medicare clearly states they are going to use physician documentation of the "reasonable basis for the expectation of a stay crossing 2-midnights" that will justify the medical necessity of the inpatient admission. If this isn't an entry into the Inpatient Social Admit Marathon, then you're not reading what I'm reading. Social admits ALWAYS take longer than two midnights to disposition out of the hospital. If a hospitalist states on admission that they think their admission for too-slothy-to-support-themselves is going to be in the hospital longer than two midnights, all they need to do is document their supporting reasons. They state that clear as day:
"The judgement of the physician and the physician's order for inpatient admission should be based on such complex medical factors as patient history and comorbidities, the severity of signs and symptoms, current medical needs and the risk of an adverse event."
"Ask your hospitalist today if mom is too old to hyperventilate and they'll work the system to get her a free entry into the Nursing Home Marathon paid for by Medicare."
%20you%20will%20find%20anywhere%20on%20the%20internet...)
Every social admit a hospitalist is asked to admit into the hospital could qualify for inpatient based on the expectation of the process taking longer than two midnights to provide an appropriate discharge to the community (especially at really crappy hospitals) and documenting their judgement of risk for an adverse event if they are not discharged to a nursing facility. They way I see it, Medicare is telling me I can qualify my 98 year old patient who is too-weak-to-hyperventilate as inpatient status by simply writing the following statement:
It is my medical judgement that Mrs Smith presents as a great danger to herself if not continuously monitored in a 24 hour care setting. Due to ___________________ (write anything reasonable that doesn't seem related to patient or family convenience) I do not expect Mrs Smith to be discharged in less than two midnights.What are the reasons social admits always take longer than two midnights to discharge? Just off the top of my head, here are some reasons:
- It's the weekend and everyone knows nursing homes don't accept new SNF patients on the weekend.
- It's a holiday. See above.
- The patient is homeless and can't find their Medicare card.
- The patient is drunk. It takes two days to safely get them sober.
- The patient refuses to be discharged and files an appeal. You get two midnights right there.
- It takes two midnights to get the psychiatrist to see the patient to tell you they can't make their own decisions.
- Any patient admitted after 6 pm by the night hospitalist isn't going to get discharged before 6 pm the next day. That's because they'll be done rounding at 9 am and all the tests won't get done until the afternoon and that means another midnight waiting for test results.
- The powers of attorney won't return your phone calls.
- It takes two midnights for families to choose a nursing home.
- Families demand 12 consultants to prove grandma is just old and weak.
- There is no access to clinic records on weekends.
- Home medications can't be verified until after the patient is already discharged.
- Physical therapists are too busy to see them on day one. Bam! You got another midnight.
- The powers of attorney is crazy themselves.
The patient won't talk to you orYou won't talk to them because they are too hard of hearing.
- Tell families to go home and don't answer their cell phone for two midnights. Don't call me. I'll call you.
- Tell families to tell the hospitalist grandpa was hallucinating this morning, although nobody saw it. Make sure to refuse the CT of the head your hospitalist will order. Delirium will buy you a midnight, maybe two.
- Order a cardiac stress test after the patient has has their morning coffee. Oops. Sorry about that. I guess they'll have to wait another midnight to get their test.
- Place them on telemetry. Note the one beat run of VT, but forget to call for a cardiology consult until late in the day on a Friday night.
- If you admit a patient on Friday, just forget to request clinic records until Saturday. That buys you the weekend while you wait for their clinic to open on Monday. It's not safe to discharge the patient without a complete picture of their health.
- Order lots of lab tests. Don't follow up on them until the next day. Regardless of what the labs show, order an advanced imaging test, but don't follow up on the results until the next day. Bam. Two midnights.
- Just order a bone marrow biopsy on a weekend to prove grandma doesn't have a case of disseminated it-just-doesn't-matter. Nobody does bone marrow biopsies on weekends. Cancel the bone marrow biopsy on Monday after confirming the patient's case of it-just-doesn't-matter.
Just wait until the general public gets a hold of this change. No longer do they need to worry about caring for grandma at home. Just bring them to the adult humane society (aka the ER), get them their two midnights on the way to the mandatory three SNF midnights and it's a Friday night SNF party at the fancy nursing home with skilled nurses. Once hospitalists get past that second midnight with inpatient status while ruling out occult bacteremia in the absence of fever, absence of leukocytosis and the absence of standard of care, they can easily get their third SNF midnight by documenting their need to confirm acute exacerbation of needs-three-midnights-and-a-place-to-live-upon-discharge.
Alternatively, I'm fascinated by all the acute drug overdose patients who require ventilator support in the ICU that are admitted at 1 am and are discharged by 3 pm. Apparently, they aren't in the hospital long enough to be admitted inpatient if the hospitalist believes they can be discharged before the following night. Apparently, they are only being observed on the ventilator to determine whether or not to actually turn the ventilator on. Being sick on the ventilator for less than one midnight just doesn't cut it anymore. If you want to qualify your critically ill drug overdose for inpatient, you'd best consider telling the family to go home and get more drugs to double the suicide dose so the hospitalist doesn't extubate them too soon from life support. It's a matter of life or 2-midnights.
However, If hospitalists document their confidence in their excellent care team and can get their critically ill patient discharged in less than two midnights, their hospital may be punished. They should instead consider providing suboptimal care, generate an iatrogenic critical medication error or two and delay the discharge past the second midnight to verify payment under inpatient status. Or maybe they should just delay their discharge for another midnight so their clearly obvious inpatient care gets paid for as an inpatient and not the less funded observation rate.
Yes folks, Medicare gave hospitalists the 3-midnight rule. Now they are preparing to give hospitalists the 2-midnight and 1-midnight rules. On October 1st, 2013, how hospitalists document their social admits will provide a great opportunity for them to show value where none previously existed. Turn that observation frown upside down and give your 108 year old with a mild case of too-old-to-calculate-her-age-based-on-her-date-of-birth a golden ticket to inpatient status and one small midnight away from the dream SNF of her choice. You owe it to her. She's 108 years old and you're not.
Some of this post is for entertainment purposes only and likely contains humor only understood by those in a healthcare profession. Read at your own risk. Including the hundreds of original Happy Hospitalist crude medical ecards on Pinterest.
Tweet
Tidak ada komentar:
Posting Komentar