Citizens who claim Obamacare is a major victory for patients are going to be greatly disappointed to learn that Obamacare promises to provide health care insurance without health care access. Obamacare promises to massively expand Medicaid. Medicaid is broke. The only places accepting Medicaid these days are hospitals and emergency rooms. I have been a practicing hospitalist now for ten years. I have seen Medicaid failures first hand. In my community of Lincoln, NE, finding a new doctor to accept Medicaid is nearly impossible. In fact, I have witnessed first hand how difficult it is to get a hospitalized patient of mine with Medicaid to find a primary care physician post hospital stay to establish new patient care. It took over 35 phone calls to over 35 clinics to find one physician's office willing to accept a new Medicaid patients. In fact, one office even required five years worth of records and an interview appointment before they would consider accepting a new Medicaid patient.
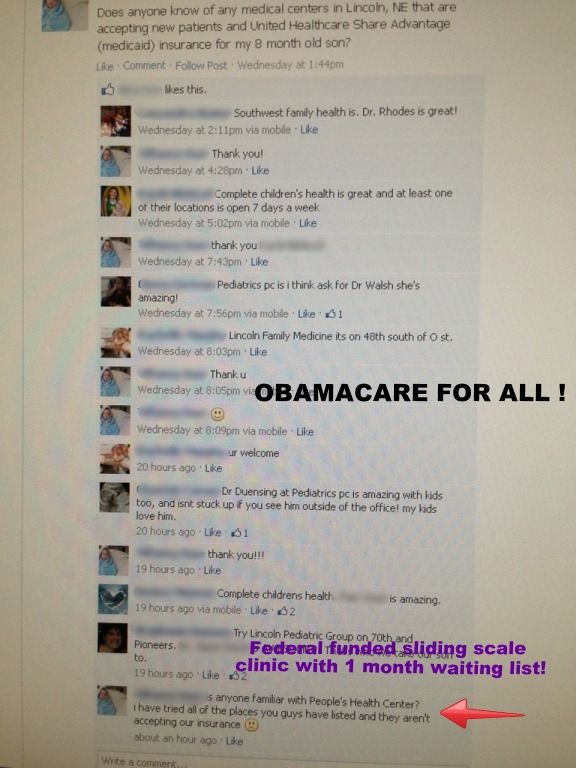
That's thirty five calls to physicians before one would accept a new Medicaid patient. ObamaCare promises to massively expand Medicaid and promises to cover some of the expansion with unstable federal money that will surely be held hostage by party politics. Physicians aren't biting. Most physicians can easily fill their schedules with follow up appointments of their other chronic disease patients. For many doctors' offices, accepting new Medicaid patients are not in their budget or long term business plan. It's not just internists and family medicine physicians that are not accepting new Medicaid patients. It's also our colleagues in the pediatric world. I was recently shown a Facebook screen shot of a woman who was looking for a pediatrician for their eight month old child with United Healthcare Share Advantage Medicaid insurance.
This is the same company I have have problems as a hospitalist getting inpatient status approved on patients who have spent less than 24 hours in the hospital (due to our excellent care), but meet inpatient criteria by all objective standards. What I saw was sad, but not shocking. Why should physicians be expected to accept insurance that costs them money every time an appointment is made. I recently wrote a Facebook comment about a physician in my community who said they make $1 for every Medicaid appointment. If they saw four Medicaid patients in an hour, they would only make $4 an hour. They said they don't work for $4 an hour. I am sad for this woman and her child. Their hearts must be broken just trying to find a physician to be her child's doctor. They must think all these great doctors are greedy for not accepting Medicaid. Many people have no idea just how badly Medicaid pays.
It's not the doctor's fault Medicaid pays so poorly that they have to turn away innocent eight month old children in favor of other commercial payers with more reasonable rates. It's no wonder why so many other citizens are opposed to Obamacare. The idea of universal access to insurance does not equate to universal access to doctors. I think emergency rooms had better get prepared for a rapid rise in new patients with Medicaid insurance but no outpatient doctor willing to see them. Why don't doctors accept Medicaid? Running a doctor's office is a business. Doctors can't treat anyone if they can't pay their bills. Hugs and thank yous don't pay the office electric bills. The future of Obamacare is here and now, but it's going to get a lot worse by making bad policy worse. Click on the Facebook screen shot below for a good look at the pain.
That's thirty five calls to physicians before one would accept a new Medicaid patient. ObamaCare promises to massively expand Medicaid and promises to cover some of the expansion with unstable federal money that will surely be held hostage by party politics. Physicians aren't biting. Most physicians can easily fill their schedules with follow up appointments of their other chronic disease patients. For many doctors' offices, accepting new Medicaid patients are not in their budget or long term business plan. It's not just internists and family medicine physicians that are not accepting new Medicaid patients. It's also our colleagues in the pediatric world. I was recently shown a Facebook screen shot of a woman who was looking for a pediatrician for their eight month old child with United Healthcare Share Advantage Medicaid insurance.
This is the same company I have have problems as a hospitalist getting inpatient status approved on patients who have spent less than 24 hours in the hospital (due to our excellent care), but meet inpatient criteria by all objective standards. What I saw was sad, but not shocking. Why should physicians be expected to accept insurance that costs them money every time an appointment is made. I recently wrote a Facebook comment about a physician in my community who said they make $1 for every Medicaid appointment. If they saw four Medicaid patients in an hour, they would only make $4 an hour. They said they don't work for $4 an hour. I am sad for this woman and her child. Their hearts must be broken just trying to find a physician to be her child's doctor. They must think all these great doctors are greedy for not accepting Medicaid. Many people have no idea just how badly Medicaid pays.
It's not the doctor's fault Medicaid pays so poorly that they have to turn away innocent eight month old children in favor of other commercial payers with more reasonable rates. It's no wonder why so many other citizens are opposed to Obamacare. The idea of universal access to insurance does not equate to universal access to doctors. I think emergency rooms had better get prepared for a rapid rise in new patients with Medicaid insurance but no outpatient doctor willing to see them. Why don't doctors accept Medicaid? Running a doctor's office is a business. Doctors can't treat anyone if they can't pay their bills. Hugs and thank yous don't pay the office electric bills. The future of Obamacare is here and now, but it's going to get a lot worse by making bad policy worse. Click on the Facebook screen shot below for a good look at the pain.
.)
Facebook universe commentary:
One thing that frustrates health care professionals is bending over backward to provide service above beyond the call of duty, often uncompensated, and then have patients flip them the bird while walking out the door waving their Medicaid card in contempt. We all end up paying for this chronic nonsense because personal responsibility is not required once this golden ticket to the waste land is "earned". The sad thing is, people who really could benefit from social safety nets can't get a doctor to take their Medicaid because system abusers have ruined it for everyone.
What doctor in their right mind would sign up for $.10 on the dollar? Their clinic would shut down in a month. I make $1 on every Medicaid patient I see in the clinic. If I see four Medicaid patients an hour, I make $4 an hour. I don't work for $4 an hour.
---Physician speaking the truth about not accepting Medicaid
Tweet
...)


%20For%20High%20Risk%20Medical%20Decision%20Making%20(MDM)%20in%20E%2FM%20Explained.)