This lecture will assist physicians and non-physician practitioners (NPP) determine if their inpatient hospital follow-up note documentation meets criteria for a level 2 (CPT® 99232 mid level subsequent care) or a level 3 (CPT® 99233 high level subsequent care) evaluation and management (E/M) code. Recovery Audit Contractors will most likely continue to target E/M codes for improper payments. Physicians and NPP must pursue documentation education to prevent accusations of over billing and to prevent under billing for work provided. I am an internal medicine physician with over 10 years experience as a clinical Hospitalist. Based on my decade of experience and exhaustive review of E/M coding criteria, I believe many level 2 hospital follow-up notes would qualify for a level 3 follow-up note if practitioners understood how to document work already being provided. The link above provides free access to dozens of billing and coding lectures I have written to help others quickly decipher the complex rules used to determine the correct CPT® code for most inpatient and outpatient hospital and clinic encounters.

 The American Medical Association's 2015 Standard Edition CPT® provides definitions of all E/M services. This valuable resource is available through Amazon by clicking on the image to the right. I have previously discussed level two inpatient subsequent care (99232) and level three inpatient subsequent care (99233) codes in detail and I recommend all readers thoroughly review these lectures at their convenience. Remember, for hospital follow-up notes, only 2 out of 3 elements from history, physical examination and medical decision making must meet criteria for the level of care to be correctly determined. This is unlike initial hospital care visits (CPT® 99221-99223 and 99218-99220) that require all three elements to meet minimum documentation criteria.
The American Medical Association's 2015 Standard Edition CPT® provides definitions of all E/M services. This valuable resource is available through Amazon by clicking on the image to the right. I have previously discussed level two inpatient subsequent care (99232) and level three inpatient subsequent care (99233) codes in detail and I recommend all readers thoroughly review these lectures at their convenience. Remember, for hospital follow-up notes, only 2 out of 3 elements from history, physical examination and medical decision making must meet criteria for the level of care to be correctly determined. This is unlike initial hospital care visits (CPT® 99221-99223 and 99218-99220) that require all three elements to meet minimum documentation criteria.
TIME
The CPT® definitions also provide guidance on expected time for the encounter. However, time can only be used in conjunction with the rules of counseling and coordination of care. Time based billing has been discussed elsewhere on The Happy Hospitalist and is not relevant to this discussion.
Appendix C of the CPT® manual provides pages and pages of clinical examples for a level 2 and level 3 hospital inpatient subsequent care visit. These examples are a tragic example of failure to appreciate the complexities of patient care. These one and two sentence scenarios cannot tell the whole picture nor do they represent the reality and complexity of patient encounters in real life. I provide two Internal Medicine examples below from the CPT® handbook.
Level 2 Subsequent Hospital Care (99232)
Level 3 Subsequent Hospital Care (99233)
As stated above, the audit components of a level 2 and a level 3 inpatient or observation hospital admission are exactly the same with the exception of the medical decision making (MDM) component. Unfortunately, this is not true for hospital follow-up visits. The history, physical examination and medical decision making components all have different documentation requirements. While CPT® definitions include reference to the stability of the patient, response to therapy or development of new complications, these factors are rarely used independently of the Marshfield Clinic audit tool rules to define the appropriate level of documentation. Many complex patients with multiple comorbidities may contain all the documentations elements necessary to achieve level 3 hospital follow-up status despite the lack of new complications or decreased stability. Great medical care that prevents deterioration in the patient condition should not be used to down charge high complexity care provided by practitioners. Based on the CPT® definitions, audit decisions are decided with a detailed analysis of history, examination and medical decision making documentation.
An auditor, who may have no medical training, must rely on tools that reliably determine the appropriate level of care provided. Medicare's E/M Services Guide provides detailed instructions for history and physical examination elements. However, guidance for determining medical decision making complexity is vague and difficult to reproduce with consistency in an audit situation. Enter the Marshfield Audit Clinic Tool and point system that was developed to provide reproducible interpretation. After a side-by-side review of history and physical examination elements for a level 2 and level 3 hospital follow-up care note, a detailed review of the Marshfield Clinic audit tool and MDM will be provided.
Where did the Marshfield Clinic point system E/M tool come from? It was developed in the early 1990s at a 600 physician multi-site, multi-specialty, mostly office-based practice in Wisconsin where Medicare's 1995 EM guidelines were beta tested. This medical decision making point system audit tool was developed by clinic staff and their local Medicare carrier. These scoring tools never made it into the official guidelines, but are accepted as a standard audit tool by most carriers today. I have created an E/M pocket reference guide as a rapid bedside decision tool that incorporates their guidance into clinical decisions. Details of this bedside reference can be found at the link provided just above. These cards are available for purchase. All proceeds are donated to charity.
CPT® DEFINITIONS
LEVEL 2 (99232) CRITERIA
A level 2 subsequent hospital care note requires documentation of at least 2 of the following 3 components: An expanded problem focused interval history; An expanded problem focused exam; Medical decision making of moderate complexity. Usually, the patient is responding inadequately to therapy or has developed a minor complication (25 minutes).
LEVEL 3 (99233) CRITERIA
A level 3 subsequent hospital care note requires documentation of at least 2 of the following 3 components: A detailed interval history; A detailed examination; Medical decision making of high complexity. Usually, the patient is unstable or has developed a significant complication or a significant new problem (35 minutes).Unlike the minor differences between a level 2 and level 3 H&P, documentation requirements between the level 2 and level 3 hospital follow-up note are significantly different and will be reviewed below.
TIME
The CPT® definitions also provide guidance on expected time for the encounter. However, time can only be used in conjunction with the rules of counseling and coordination of care. Time based billing has been discussed elsewhere on The Happy Hospitalist and is not relevant to this discussion.
CLINICAL EXAMPLES
Appendix C of the CPT® manual provides pages and pages of clinical examples for a level 2 and level 3 hospital inpatient subsequent care visit. These examples are a tragic example of failure to appreciate the complexities of patient care. These one and two sentence scenarios cannot tell the whole picture nor do they represent the reality and complexity of patient encounters in real life. I provide two Internal Medicine examples below from the CPT® handbook.
Level 2 Subsequent Hospital Care (99232)
Subsequent hospital care visit for a 62-year-old female with congestive heart failure, who remains dyspneic and febrile.CPT® provides this scenario as an appropriate level 2 subsequent care visit. I disagree. Most patients in this situation with multiple other comorbidities would clearly qualify for medical decision making of high complexity based on the Marshfield Clinic audit tool (described in detail below). In addition, a level 3 history and physical examination would be medically indicated for this clinically complex situation with a broad differential diagnosis. This clinical description in CPT® 2014inappropriately fails to recognize the risk and complexity of inpatient hospital care. These CPT® clinical examples are not representative of real life patients. Most patients do not present with single diseases. Their complexity rises exponentially with other comorbid conditions. I do not place faith on these CPT® examples for providing appropriate coding guidance. This is why alternative methods have been developed to define moderate and high complexity and risk in audit situations. Here is a 2014 CPT® handbook example of a level 3 subsequent hospital care.
Level 3 Subsequent Hospital Care (99233)
Subsequent hospital visit for a type 1 diabetes mellitus patient with a new onset of fever, change in mental status, and a diffuse petechial, purpuric eruption.I agree. However, I also believe a higher percentage of hospital subsequent care visits are complex enough to warrant level 3 coding independent on the patient's clinical response to treatment. A patient need not always be failing treatment or be unstable to meet criteria for level 3. For example, patients with HTN, COPD, DM and a new onset stroke on a heparin drip with frequent lab draws for drug management should be appropriately be billed as a high level 99233 for many days, independent of the patient's clinical response to treatment or the development of complications. The Marshfield Clinic audit tool provides support for this statement. Physicians have an obligation to accurately describe variables which provide coding audit personnel a rationale to support high complexity coding decisions.
COMPARISON BETWEEN A LEVEL 2 AND LEVEL 3 FOLLOW-UP
As stated above, the audit components of a level 2 and a level 3 inpatient or observation hospital admission are exactly the same with the exception of the medical decision making (MDM) component. Unfortunately, this is not true for hospital follow-up visits. The history, physical examination and medical decision making components all have different documentation requirements. While CPT® definitions include reference to the stability of the patient, response to therapy or development of new complications, these factors are rarely used independently of the Marshfield Clinic audit tool rules to define the appropriate level of documentation. Many complex patients with multiple comorbidities may contain all the documentations elements necessary to achieve level 3 hospital follow-up status despite the lack of new complications or decreased stability. Great medical care that prevents deterioration in the patient condition should not be used to down charge high complexity care provided by practitioners. Based on the CPT® definitions, audit decisions are decided with a detailed analysis of history, examination and medical decision making documentation.
An auditor, who may have no medical training, must rely on tools that reliably determine the appropriate level of care provided. Medicare's E/M Services Guide provides detailed instructions for history and physical examination elements. However, guidance for determining medical decision making complexity is vague and difficult to reproduce with consistency in an audit situation. Enter the Marshfield Audit Clinic Tool and point system that was developed to provide reproducible interpretation. After a side-by-side review of history and physical examination elements for a level 2 and level 3 hospital follow-up care note, a detailed review of the Marshfield Clinic audit tool and MDM will be provided.
HISTORY: LEVEL 2 VS. LEVEL 3
The history requirements for a 99232 and 99233 encounter are quite different. Required elements can be reviewed on pages 26-30 of Medicare's E/M Services Guide. Here is a summary of those requirements:
LEVEL 2 HISTORY
HPI: 1-3 elements or documentation of the status of three chronic medical conditions
ROS: 1 or more systems
PMFSH: None
LEVEL 3 HISTORY
HPI: 4 or more elements or documentation of the status of three chronic medical conditions
ROS: 2-9 systems
PMFSH: None
PHYSICAL EXAMINATION: LEVEL 2 VS. LEVEL 3
The physical examination requirements for a 99232 and 99233 encounter are quite different. Required elements can be viewed on page 31 (for 1995 guidelines) page 49 (1997 guidelines) of Medicare's E/M Services Guide.
LEVEL 2 PHYSICAL EXAMINATION
1995 guidelines: a limited examination of the affected body area or organ system and other symptomatic or related organ system(s).
1995 guidelines: a limited examination of the affected body area or organ system and other symptomatic or related organ system(s).
1997 guidelines: a limited examination of the affected body area or organ system and any other symptomatic or related body area(s) or organ system(s). 1997 guidelines allow for a multi-system exam (described on page 13 of the E/M Services Guide) or a single organ exam (described on page 18 of the E/M Services Guide). A general multi-system exam should include performance and documentation of at least six elementsidentified by a bullet (•) in one or more organ system(s) or body area(s). A single organ system exam should include performance and documentation of at least six elementsidentified by a bullet (•) in one or more organ system(s) or body area(s).
LEVEL 3 PHYSICAL EXAMINATION
1995 guidelines: an extended examination of the affected body area(s) and other symptomatic or related organ system(s).
1997 guidelines: an extended examination of the affected body area(s) or organ system(s) and any other symptomatic or related body area(s) or organ system(s). 1997 guidelines allow for a multi-system exam (described on page 13 of the E/M Services Guide) or a single organ exam (described on page 18 of the E/M Services Guide). A general multi-system exam should include at least six organ systems or body areas . For each system/area selected, performance and documentation of at least two elements identified by a bullet (•) is expected. Alternatively, a detailed examination may include performance and documentation of at least twelve elements identified by a bullet (•) in two or more organ systems or body areas. A single organ system exam, other than the eye and psychiatric examinations, should include performance and documentation of at least twelve elementsidentified by a bullet (•), whether in a box with a shaded or unshaded border. Eye and psychiatric examinations should include the performance and documentation of at least nine elements identified by a bullet (•), whether in a box with a shaded or unshaded border.
MEDICAL DECISION MAKING (MDM): LEVEL 2 VS. LEVEL 3
MARSHFIELD CLINIC AUDIT TOOL
Where did the Marshfield Clinic point system E/M tool come from? It was developed in the early 1990s at a 600 physician multi-site, multi-specialty, mostly office-based practice in Wisconsin where Medicare's 1995 EM guidelines were beta tested. This medical decision making point system audit tool was developed by clinic staff and their local Medicare carrier. These scoring tools never made it into the official guidelines, but are accepted as a standard audit tool by most carriers today. I have created an E/M pocket reference guide as a rapid bedside decision tool that incorporates their guidance into clinical decisions. Details of this bedside reference can be found at the link provided just above. These cards are available for purchase. All proceeds are donated to charity.
LINK TO E/M POCKET REFERENCE POST
|

CMS GUIDANCE ON MEDICAL DECISION MAKING
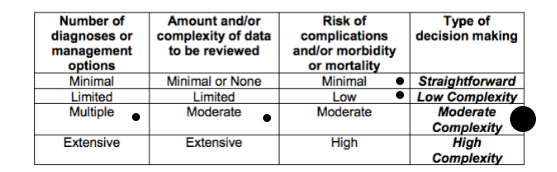
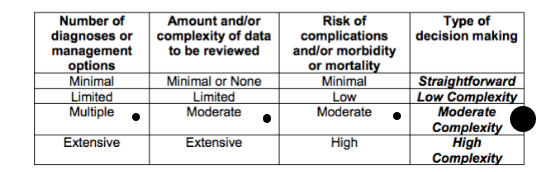
Why do many Medicare carriers use the Marshfield Clinic Audit Tool to determine the correct level of service provided? Medicare's description of medical decision making in the Evaluation and Management Services Guide (page 33) contains vague language that cannot be reliably reproduced in clinical practice. Here is a screen shot of the E/M Services Guide discussing medical decision making criteria.
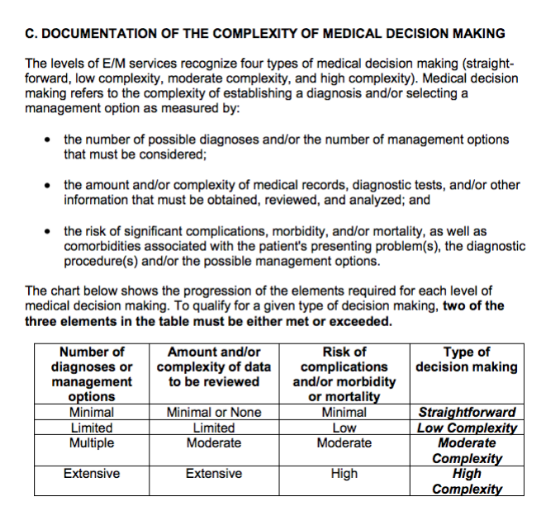
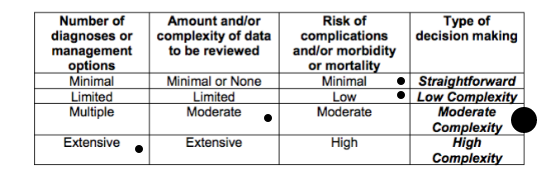
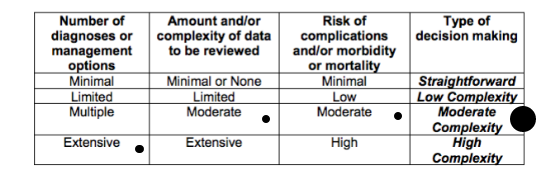
How can a practitioner or auditor reliably determine when the number of diagnoses are multiple or extensive? How can a practitioner or auditor reliably determine when the amount and complexity of data is moderate or extensive? They can't. Ironically, determining the correct level of medical decision making complexity is complex. Just as the CPT® definitions use vague language in defining their codes, the E/M Services Guide also uses the same difficult language to guide physicians and other NPPs. This is a tragic. This is why The Marshfield Clinic Audit Tool for MDM was developed and used by auditors and practitioners to stay compliant. Pages 33-37 of the E/M Services Guide provides the basis for the Marshfield Clinic Audit Tool point system shown above on The Happy Hospitalist's bedside pocket E/M reference card. It provides quick access to documentation elements converted into Marshfield Clinic Audit Tool points. It may also help providers remember to document work provided but rarely described in the chart in order to get credit for documentation elements in an audit situation. For example, in the number of diagnoses or management options component of medical decision making, three points is given for a new problem with no workup planned when using the Marshfield Clinic Audit Tool. This is based on Medicare's E/M Services Guide (page 34) description of diagnosis complexity here.
The number and type of diagnostic tests employed may be an indicator of the number of possible diagnoses. Problems which are improving or resolving are less complex than those which are worsening or failing to change as expected.This same point system applies to the amount and/or complexity of data to be reviewed. For example, one point is given for ordering a lab or an x-ray in the Marshfield Clinic Audit Tool. This decision is based on Medicare's E/M Services Guide (page 35) description of amount and/or complexity of data to be reviewed.
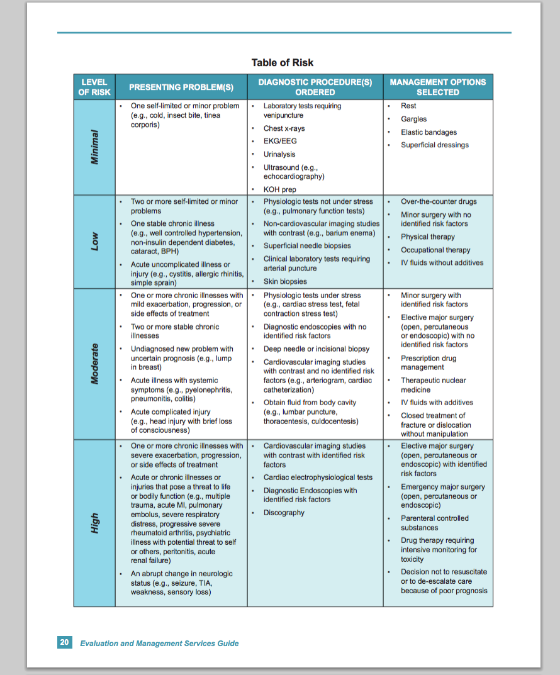
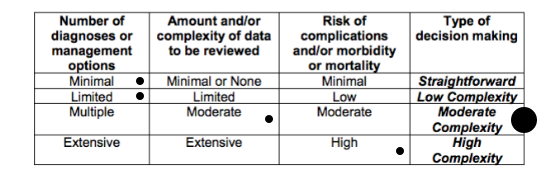
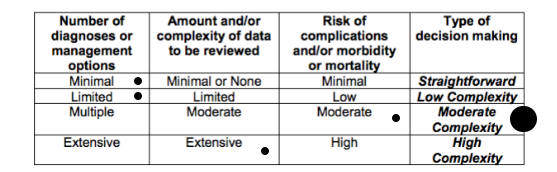
If a diagnostic service (test or procedure) is ordered, planned, scheduled, or performed at the time of the E/M encounter, the type of service, eg , lab or x -ray, should be documented.Medicare does provide decent guidance on risk of complications and/or morbidity or mortality with their risk table (shown below). However, some elements within this table contain vague language that can be open to interpretation and require physicians and other NPP to document their thought processes aggressively to avoid accusations of incorrect billing when they believe high risk to the patient is present.
SIDE-BY-SIDE MDM CRITERIA COMPARISON (Level 2 vs Level 3)
If you feel lost in this discussion, now is the time to place close attention. Using Medicare's E/M Services Guide as a reference, I have incorporated the Marshfield Clinic point system as a side-by-side reference below.
Within the diagnosis and data elements of MDM, points are provided for defined elements of documentation found during a chart audit. For example, one point is allowed for a self limiting or minor problem in the diagnosis section of MDM while one point may be given for evidence the provider requested prior records. This is the basis of the point system under the Marshfield Clinic Audit Tool that is used by most Medicare carriers.
While this point system is not officially part of Medicare's E/M Services Guide, the risk table is. The risk table is available on page 20 or 37 of the Evaluation and Management Services Guide. I have provided a screen shot here for quick reference. The highest element anywhere on the risk table determines the highest overall level of risk on the risk table. For example, a patient with an abrupt change in neurological status meets criteria for high risk on the risk table regardless of any other data points on the table.
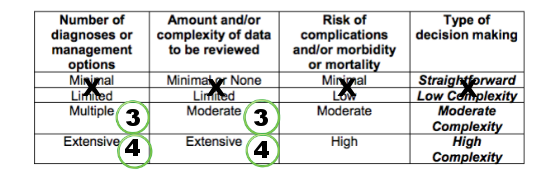
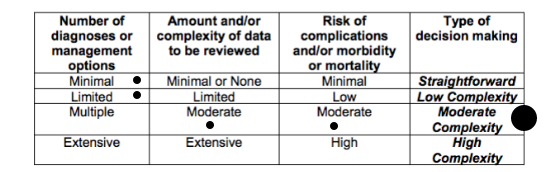
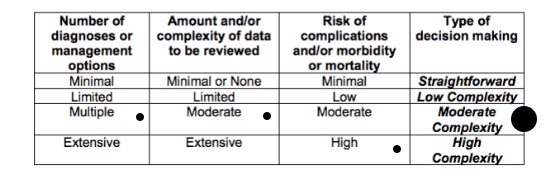
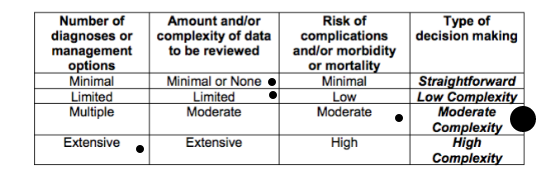
To determine the overall level of MDM complexity, the highest two out of three elements from diagnoses, data and risk determine the overall level of MDM. In other words, the highest level of documentation for data and diagnosis, data and risk or diagnosis and risk will determine the overall level of MDM. Below are the minimum MDM criteria for a level 2 and level 3 subsequent hospital care. For example a patient who's documentation supports 3 diagnosis points, 1 data point and moderate risk would qualify for level 2 MDM. A patient who's documentation supports 2 diagnosis points, 4 data points and high risk would qualify for level 3 MDM. A patient who's documentation supports 2 diagnosis points, 2 data points and high risk would not qualify for either level 2 or level 3 MDM for subsequent hospital care visit.
LEVEL 2 MDM (highest 2 out of 3 determines overall level of MDM)
DIAGNOSIS: 3 points
DATA: 3 points
RISK TABLE: moderate
LEVEL 3 MDM (highest 2 out of 3 determines overall level of MDM)
DIAGNOSIS: 4 points
DATA: 4 points
RISK TABLE: high
LEVEL 2 PERMUTATIONS
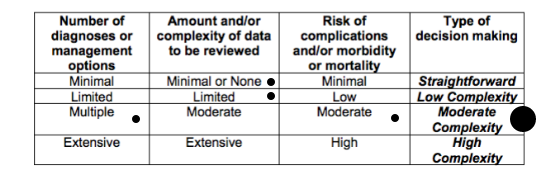
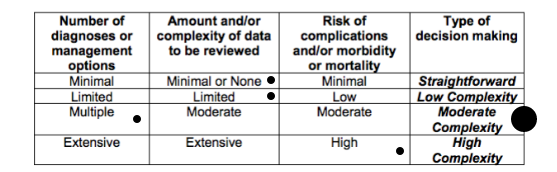
Here are all eleven potential documentation permutations for medical decision making of a level 2 subsequent hospital care evaluation. However, keep in mind subsequent hospital care evaluations only require the highest two out of three elements from history, physical examination and medical decision making. E/M rules do not mandate medical decision making as a required element. The two out three highest levels of documentation in diagnosis, data and risk will determine the overall level of MDM. If MDM is going to be used, the following graphics describe all permutations of moderate complexity medical decision making (level 2). This same exercise can be done to determine high complexity medical decision making (level 3)
Remember to always consider medical necessity. For example, ordering a head CT to increase the complexity of medical decision making on a chief complaint of pulled hamstring may raise some red flags if the chart undergoes an audit. I believe if you're anywhere in the ball park of practicing standard of care, justifying medical necessity will rarely be a determining factor in having to support your level of care based on history, physical or decision making.
WHERE CAN I GET A COPY OF THE POINT SYSTEM?
Many examples of the Marshfield Clinic point system are available on the internet. Page two of this Codeapedia reference provides a detailed description of the point system. This point system is the basis for the bedside E/M reference card provided by The Happy Hospitalist pictured above and linked here again for easy reference.
MANY LEVEL 2s ARE PROBABLY LEVEL 3s
In reality, many physicians and other NPP are scared to bill too many level 3 hospital follow-up notes for fear of getting audited. No fear should exist if documentation supports level 3 work already being provided. If all providers would document work they are already providing and billed appropriately, level 3 subsequent care distribution would rise dramatically and physician outliers, who are coding correctly, would disappear. Practitioners worried about getting audited as an outlier should continue to document work they are already providing and to bill correctly, regardless of their status as an outlier. Being an outlier is not fraudulent when documentation supports correct coding decisions. It's quite possible that most physicians who aren't billing higher levels of 99233 vs 99232 visits are the outliers because they either don't document work they are already providing, are not providing work that is medically necessary or are intentionally under billing for fear of an audit.
RVU COMPARISON
Most E/M services are given a relative value unit (RVU) value by CMS. I have previously discussed RVUs. The most updated table of RVU values can be found here. The difference in relative value units assigned to a level 2 vs. a level 3 subsequent hospital care visit are significant. For practitioners who's compensation may be determined by productivity, coding accurately for work already being provided can boost payments significantly. What are the RVU values for a level 2 and level 3 hospital follow-up? For Medicare patients in 2016, one RVU is worth $35.8043.
LEVEL 2 (99232)
- work RVU 1.39; total RVU 2.02
LEVEL 3 (99233)
- work RVU 2.0; total RVU 2.91
A level 3 hospital subsequent care visit is valued nearly 45% higher than a level 2 based on total RVU and work RVU. This difference is significant. Since subsequent hospital care visits represent a large percentage of most hospital based medical physicians, appropriately coding level 3 instead of level 2 when documentation supports those efforts would provide a significant increase in revenue opportunity.
DISTRIBUTION OF LEVEL 2 vs. LEVEL 3 HOSPITAL FOLLOW-UP
What is the distribution of level 2 and level 3 hospital admissions? This can vary depending on specialty. One Medicare carrier has provided us insight into 99232 vs 99233 coding distribution at 62% and 30% respectively. Other Medicare distribution data is available at the CPT® 99232 and CPT® 99233 articles linked near the top of this lecture. These distribution numbers confirm similarity with SHM/MGMA data.
PAYMENT COMPARISON
Payments will vary based on geographical location. Providers in New York would generally get paid more than providers in North Dakota. For example, in some localities, a level 2 subsequent hospital care visit pays around $70 and a level 3 subsequent hospital care visit around $100, a nearly 45% increase. Failure to document work already being provided can be expensive. Given the large volume of subsequent care visits provided by Hospitalists and other hospital based specialties, knowing how to document work already being provided is valuable in any practice.
RAC AUDITORS
Medicare may be targeting inappropriate payments to providers for subsequent hospital care visits. A practitioner's best defense against accusations of fraud is to document thoroughly for work provided and to practice standard of care. Despite being an outlier, accurate stand alone documentation of medically necessary care should always support any coding distribution that results. I have thoroughly reviewed Medicare's Evaluation and Management Services Guide and can confirm that fear of an audit is not an element that should be used to guide coding decisions.

Tweet
Tidak ada komentar:
Posting Komentar