This 99226 CPT® lecture reviews the procedure code definition, progress note examples, distribution and RVU values for this new since 2011 subsequent observation care evaluation and management (E/M) code. CPT stands for Current Procedural Terminology. CPT® 99226 is the highest (level 3) subsequent observation care code in this family of codes that also includes CPT® codes 99224 and 99225. All three codes are part of the Healthcare Common Procedure Coding System (HCPCS). Observation care is considered outpatient care. A patient is considered outpatient until inpatient admission to a healthcare facility occurs. This procedure code lecture for subsequent observation care is part of a complete series of CPT® lectures written by myself, a board certified internal medicine physician with over ten years of clinical hospitalist experience in a large community hospitalist program. I have written my collection of evaluation and management (E/M) lectures over the years to help physicians and non-physician practitioners (nurse practitioners, clinical nurse specialists, certified nurse midwives and physician assistants) understand the complex criteria needed to stay compliant with the Centers for Medicare & Medicaid Services (CMS) and other third party insurance companies.
You can find my entire collection of constantly updated medical billing and coding CPT® lectures together in one place on my Pinterest site (CPT® lectures here and other associated E/M lectures here). You don't need to be a Pinterest member to get access to any of my CPT® procedure lectures. As you start to understand these E/M procedure codes, remember you have an obligation to make sure your documentation supports the level of service you are submitting for payment. The volume of your documentation should not be used to determine your level of service. The details of your documentation are what matter most. In addition, the E/M services guide says the care you provide must be "reasonable and necessary" and all entries should be dated and contain a CMS defined legible signature or signature attestation, if necessary.
The Centers for Medicare & Medicaid Services (CMS) has recognized subsequent observation care codes (99224-99226) since calendar year 2011's Physician Fee Schedule (PFS) with comment period (CMS-1503-FC). CPT® codes 99224-99226 should be used by the admitting physician for day(s) other than the initial or discharge date. Consulting physicians should continue to use established outpatient care codes 99211-99215 instead for all days other than the initial encounter, in most circumstances.
My interpretations discussed below are based on my review of the 1995 and 1997 E&M guidelines, the CMS E&M guide and the Marshfield Clinic audit point system for medical decision making. These resources can be found in my hospitalist resources section. The Marshfield Clinic point system is voluntary for Medicare carriers but has become the standard audit compliance tool in many parts of the country. You should check with your own Medicare carrier in your state to verify whether or not they use a different criteria standard than that for which I have presented here in my free educational discussion. I recommend all readers obtain their own updated CPT® reference book as the definitive authority on CPT® coding. I have provided access through Amazon to the 2015 CPT® standard edition pictured below and to the right. The American Medical Association (AMA) describes the 99226 CPT® procedure code as follows:
When I come upon the chart of a patient, I want to know if there are any new issues that have presented since my last evaluation. If the answer is yes, my documentation can usually support a level three progress note. Remember, the rules are not based on how much is written, but rather what is written. If the answer is no, I review the chart and medical conditions to decide whether the patient would qualify anyway in an effort to submit accurate coding decisions everytime. I think physicians universally underestimate risk as it applies to E/M coding. Many of our patients should be categorized as high risk and billed as such if other documentation supports the highest level of medically reasonable and necessary service. Listed below are some examples of 99226 subsequent observation care notes in subjective, objective, assessment, plan (SOAP) format. A CPT® 99226 note could look like this:
Remember, medical decision making guidelines also require a determination of the highest two out of three for data, diagnosis and risk. I received high complexity medical decision making based on data and risk. I had documentation of at least 12 bullets in six organ systems on physical exam. Therefore, this note meets criteria for a CPT® 99226. One does not need to write volumes of information to meet criteria for high complexity care. While I wrote no ICD code in this note, documentation should support somewhere what the visit was for. These progress note examples are based on strict interpretation of the E/M Marshfield Clinic audit tool rules. Remember to always include medically reasonable and necessary in your evaluation decisions. Here is another example:
Is the patient worse or unstable? Not necessarily. But their complexity and risk overcome that aspect based on the Marshfield Clinic audit tool rules we have been expected to comply with. The E/M rules do not say the patient must be unstable or worse and the CPT definition does not say they must be unstable or worse. These rules were created to provide clarity for physicians and coders and auditors alike. Here is another 99226 example:
I hope these common clinical examples offer further proof that documentation is key to staying compliant. Writing a novel is not required. As physicians, I think we tend to underestimate the level of complexity we encounter because we are used to it. We need to do a better job of documenting what we do and understand the rules we have been given to follow. Notice these notes are not long essays. They are strategically written to capture value in work we are doing but not currently describing in the correct manner. Don't be afraid to bill 99226 if the face-to-face encounter you provide is medically reasonable and necessary and your documentation supports CPT® 99226. In fact, if you think about it, patients in observation may not be "sick enough" to be admitted, but CMS has instructed us to use CPT® code 99226 for high complexity observation evaluations whose criteria is exactly the same as high complexity patients who are admitted as inpatients. Being observation does not mean they are too healthy for high complexity care. Always keep in mind documentation is key to getting paid, based on the rules we have been given, for the work we are providing.
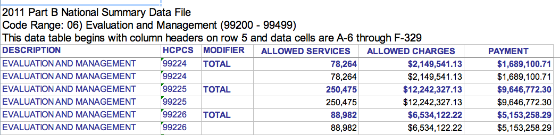
What is the distribution of CPT® code 99226 relative to other levels of service in this family of medical codes? The CPT® group 99224-99226 is pretty new. CMS has only recognized these codes since 2011. However, CMS has data explaining how often 99224, 99225 and 99226 have been used. The graphic below was obtained from the 2011 CMS Part B National Procedure Summary Files data (2011 zip file) showing how many CPT® 99226 encounters were billed and the dollar value of their services for Part B Medicare. As you can see in the image below, E/M code 99226 was billed 88,982 times in 2011 with allowed charges of $6,534,122.22 and payments of $5,153,258.29.
How much money does a CPT® 99226 pay in 2016? That depends on what part of the country you live in and what insurance company you are billing. E/M procedure codes, like all CPT® billing codes, are paid in relative value units (RVUs). This complex RVU discussion has been had elsewhere on The Happy Hospitalist. For raw RVU values, a CPT® 99226 is worth 2.96 total RVUs. The work RVU for 99226 is valued at 2.0. Make sure to review the complete list of RVU values on common hospitalist E/M codes. What is the Medicare reimbursement for CPT® code 99226? In my state, a CPT® 99226 pays just over under $100 in 2016. The dollar conversion factor for one RVU in 2014 is 35.8043.
My E/M reference card below has taught me that I should be billing for the work I'm providing and it has taught me how to document appropriately. You can see many more of my E/M lectures by clicking through on the provided link. If you need bedside help determining what level of care you have provided, I recommend reviewing the pocket card described below.
You can find my entire collection of constantly updated medical billing and coding CPT® lectures together in one place on my Pinterest site (CPT® lectures here and other associated E/M lectures here). You don't need to be a Pinterest member to get access to any of my CPT® procedure lectures. As you start to understand these E/M procedure codes, remember you have an obligation to make sure your documentation supports the level of service you are submitting for payment. The volume of your documentation should not be used to determine your level of service. The details of your documentation are what matter most. In addition, the E/M services guide says the care you provide must be "reasonable and necessary" and all entries should be dated and contain a CMS defined legible signature or signature attestation, if necessary.
99226 MEDICAL CODE DESCRIPTION
The Centers for Medicare & Medicaid Services (CMS) has recognized subsequent observation care codes (99224-99226) since calendar year 2011's Physician Fee Schedule (PFS) with comment period (CMS-1503-FC). CPT® codes 99224-99226 should be used by the admitting physician for day(s) other than the initial or discharge date. Consulting physicians should continue to use established outpatient care codes 99211-99215 instead for all days other than the initial encounter, in most circumstances.
My interpretations discussed below are based on my review of the 1995 and 1997 E&M guidelines, the CMS E&M guide and the Marshfield Clinic audit point system for medical decision making. These resources can be found in my hospitalist resources section. The Marshfield Clinic point system is voluntary for Medicare carriers but has become the standard audit compliance tool in many parts of the country. You should check with your own Medicare carrier in your state to verify whether or not they use a different criteria standard than that for which I have presented here in my free educational discussion. I recommend all readers obtain their own updated CPT® reference book as the definitive authority on CPT® coding. I have provided access through Amazon to the 2015 CPT® standard edition pictured below and to the right. The American Medical Association (AMA) describes the 99226 CPT® procedure code as follows:
This medical billing code can be used to bill based on time when certain requirements are met. However, documentation of time is not required to remain compliant with CMS regulations. If billed without time as a consideration, CPT® 99226 documentation should comply with the rules established by the 1995 or 1997 guidelines referenced above. The three important coding components for a subsequent observation care evaluation are:Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history; a detailed examination; medical decision making of high complexity. Counseling and/or coordination of care with other clinicians or agencies is provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Typically, 35 minutes are spent at the bedside and on the patient's hospital floor or unit.

- History
- Physical Exam
- Medical Decision Making Complexity (MDM)
- Detailed interval history: Requires four elements of the history of present illness (HPI) or documentation of the status of three chronic medical conditions. Two review of systems (ROS) are also required. No past medical history or family history or social history is required (PMFSH).
- Detailed physical exam:
- 1995 E/M guidelines require an extended exam of the affected body area(s) and other symptomatic or related organ systems. These terms are poorly defined and I feel they are open to great variation of interpretation. Note the wordage difference with body area vs organ systems. They are not the same. A review of the acceptable body areas and organ systems can be found in the CMS E&M reference guide on pages 31 and 32. I recommend instead to consider using the 1997 guidelines that provide better clarity.
- 1997 E/M guidelines more clearly define the need for a physical exam that includes at least six areas with two bullets each, or two plus areas with 12 total bullets.
- High complexity medical decision making (MDM): This is split into three components. The two out of the three highest levels in MDM are used to determine the overall level of MDM. The level is determined by a complex system of points and risk. What are the three components of MDM and the minimum required level of points and risk as defined by the Marshfield Clinic audit tool for high complexity MDM?
- Diagnosis (four points)
- Data (four points)
- Risk (high) The table of risk can be found on page 37 of the CMS E&M reference guide.
CLINICAL EXAMPLES OF CPT® 99226
Here are my general thoughts on billing a 99226 followup note: They almost always have some sort of new issue going on. That's a general rule I use when trying to decide whether or not to code this level, but that's by no means always the case. When billing this level three note, I usually try and include medical decision making in my coding decision. As I said above, MDM is not required because only two out of three for history, physical and MDM must qualify for a level three 99226. However, I feel, if I am doing a physical exam that warrants 12 bullet points, it's because they have an issue or are sick enough to qualify for the highest MDM category. With that said, this may not always be the case. For example, a patient with acute or chronic multiple organ failure may require extensive daily physical exam that requires at least 12 bullet points for medically necessary care. Evaluation and management "check list" rules allow history and physical documentation to determine the overall level of care for observation follow-up care notes.
In this example history (subjective) and physical (objective) meet the requirements to get paid for a 99226. Remember, the highest two out of three components determine the highest level of service for subsequent observation care visits. Do note that linking an ICD code to a CPT® code is required for all visits submitted for reimbursement to CMS. Most progress notes should provide at least one ICD code to clearly indicate a purpose for the visit. I suspect this is necessary to meet the reasonable and necessary threshold, unless that can be inferred from other chart documentation. Medicare doesn't want to pay for doctors just to talk about the Super Bowl with their patients.S) RLQ abdominal pain, sharp, started yesterday, constant (4 HPI)no CP, no SOB (2 ROS)O) 120/80 80 Tm 98.6n (3 vitals is 1 organ)Alert, anxious, regular rhythm, normal femoral pulses, lungs clear, normal respiratory effort, bowel tones present, no tenderness, no palpable abdominal masses, no peritonitis signs, no clubbing, no synovitis, no rash (6 areas, 12 bullets)A) nothing neededP) nothing needed
Some folks may argue that MDM must be included as one of the three components for this high level E/M visit. The rules and guidelines we are asked to follow do not state that. They clearly say that two out of three from history, physical and medical decision making determine the overall level of care. They do no state medical decision making must be one of the components. Some may argue that 12 bullet points are not medically necessary without high complex medical decision making. As a practicing hospitalist of over ten years, I would consider that assumption to be inaccurate. Every patient presents with their own special circumstances and a blanket statement about the extent of a physical exam needing to correlate with medical decision making has never been defined for us. Again, I encourage using MDM as one of the two elements in determining the overall level of care, but the rules do not state this to be necessary.
There are many patients that require intensive physical exam that may not have criteria for high complexity MDM. Documentation is vitally important to avoid any questions in an audit situation. If you feel an extensive physical exam is warranted everyday, document your reasoning why. That's what determines medically reasonable and necessary care. And always remember, when submitting payment to CMS, documentation must support at least one ICD (the problem) code from which to link the CPT® code to. I usually recommend documenting at least one problem in the note, unless the problem can be inferred elsewhere in the chart (such as in the orders as an indication for a test). Here's another example of a level three subsequent observation progress note below:
In this progress note example a level three is achieved based on documentation bullets from the physical exam and medical decision making. Nothing is needed from the history component. Remember, two out of three for subsequent observation care documentation. I documented a 99226 in the medical decision making because I achieved four points in the data section with two points for discussing with Dr Smith and two points for personally reviewing the CXR. I also got high risk for drug therapy requiring intensive monitoring for toxicity. Coumadin is a drug that I follow for toxicity by drawing INR levels. I think Coumadin use in the hospital is high risk, under most circumstances, and I make sure my documentation supports my thought processes on why I consider it so. S) no CP, no SOB (2 ROS)O) 120/80 80 Tm 98.6 (3 vitals as 1 organ system)Alert, anxious, regular rhythm, normal femoral pulses, lungs clear, normal respiratory effort, bowel tones present, no abdominal bruit, no tenderness, no clubbing, no synovitis, no rash (6 areas, 12 bullets)A) HTN-stable, no changes planned (status of 3 chronic medical conditions)COPD-stable, no changes plannedCAD-stable, no changes plannedP) Nothing needed
Again, this progress note meets criteria for a high level (level 3) based on history and physical exam. However, in this case, the status of three chronic medical conditions (which have relevance to the patient's condition) substitute for four elements of HPI. Documenting stable HTN, CAD and COPD with no changes planned is considered an appropriate substitute for four HPI elements. I would only consider using chronic conditions that have relevance to the patient's condition. Again, if there is any question about their relevance, document your thought process. The reason many physicians fail audits is not because they are committing fraud but rather because they commit omissions of documentation. They fail to explain their reasoning behind their decisions. Here is another high level progress note below:
S) Nothing neededO) 120/80 80 Tm 98.6 (3 vitals is 1 organ)Alert, anxious, regular rhythm, normal femoral pulses, lungs clear, normal respiratory effort, bowel tones present, no tenderness, no clubbing, no synovitis, no rash (6 areas, 12 bullets)Labs INR 1.7 on Coumadin (high risk for drug management requiring intensive monitoring for toxicity). CXR film personally reviewed-normal (2 points-Data for personal review of CXR). Discussed antibiotic options with Dr Smith. (2 points-Data for discussion of case with another healthcare provider).A) Nothing neededP) Nothing needed.
Remember, medical decision making guidelines also require a determination of the highest two out of three for data, diagnosis and risk. I received high complexity medical decision making based on data and risk. I had documentation of at least 12 bullets in six organ systems on physical exam. Therefore, this note meets criteria for a CPT® 99226. One does not need to write volumes of information to meet criteria for high complexity care. While I wrote no ICD code in this note, documentation should support somewhere what the visit was for. These progress note examples are based on strict interpretation of the E/M Marshfield Clinic audit tool rules. Remember to always include medically reasonable and necessary in your evaluation decisions. Here is another example:
This note meets a high level 99226 progress note based on physical exam and MDM again. History does not matter here. The physical exam achieves level three based on 12 bullets in at least six areas. The MDM is high complexity based on the diagnosis and risk components. Documentation supports four points for documenting four stable chronic medical conditions with AF, HTN, DM and CHF. You get high risk for documenting high risk drug management with warfarin. This is a level three progress note. The care and documentation is medically reasonable and necessary. These are hospitalist patients that I feel we under code every day because we fail to appreciate how complex they are and we fail to document work we are already doing to indicate complexity.S) nothing neededO) 120/80 80 Tm 98.6 (3 vitals is one organ)Alert, anxious, regular rhythm, normal femoral pulses, lungs clear, normal respiratory effort, bowel tones present, no tenderness, no clubbing, no synovitis, no rash (at least 6 areas, 12 bullets)A) 1) Afib, rate controlled, improved, on Coumadin, INR 1.7 (High risk for drug therapy requiring intensive monitoring for toxicity)2) Acute HTN, improved (4 points for Diagnosis for 4 stable conditions)3) Uncontrolled DM, improved4) Acute systolic HF, improvedP) Nothing needed
Is the patient worse or unstable? Not necessarily. But their complexity and risk overcome that aspect based on the Marshfield Clinic audit tool rules we have been expected to comply with. The E/M rules do not say the patient must be unstable or worse and the CPT definition does not say they must be unstable or worse. These rules were created to provide clarity for physicians and coders and auditors alike. Here is another 99226 example:
This is a high level subsequent observation care progress note based on physical exam and MDM. The physical exam has at least 12 bullet points in six areas. The MDM is high complexity based on diagnosis and risk. Four points is given for addressing a new issue with further workup planned. In addition, this note provides high risk for drug therapy requiring intensive monitoring for toxicity. This is a level three progress note. Do you see how compact the note is? What is written is what matters. How much is written does not determine the level of care because documentation guidelines do note state how long your note is determines the level of care. Here is another example of a 99226 progress note:S) nothing neededO) 120/80 80 Tm 98.6 O2 86% RA (at least 3 vitals is one organ)Alert, anxious, regular rhythm, normal femoral pulses, lungs clear, no crackles, no wheezes, normal chest wall motion, no JVD, normal respiratory effort, bowel tones present, no tenderness, no clubbing, no synovitis, no rash (at least 6 areas, 12 bullets)INR 1.7 on Coumadin (High risk for drug management requiring intensive monitoring for toxicity)A) hypoxemia-new issue (Diagnosis-4 points for new problem with further workup planned)P) get CXR, ABG
Level three is achieved using history and MDM. The history qualifies for a 99226 based on four HPI and two ROS elements. The MDM qualifies based on diagnosis and risk. Four diagnosis points is given for a new problem with further workup planned. High risk for Coumadin management. Did you ever think you could write so little and still bill an appropriate 99226 based on the audit tool E/M guidelines physicians are expected to follow? Here is another example using history and MDM:S) RLQ abdominal pain, sharp, started yesterday, constant (4 HPI)no CP, no SOB (2 ROS)O) nothing neededINR 1.7 on Coumadin (high risk drug management)A) hypoxemia-new (Diagnosis-4 points for new problem with further workup)P) Check ABG, CXR
In this example, the status of three chronic medical conditions substitutes for the four HPI elements. The MDM is high complexity for risk and diagnosis. Discussing DNR and writing an order for such can qualify for high risk under the risk table guidelines. In addition, four points under diagnosis of a new medical condition with further workup planned meets high complexity care criteria. This is a high level 99226 progress note. The following progress note is one last example of a CPT 99226 based on history and MDM:S) no CP, no SOB (2 ROS)O) Nothing neededA) 1) DM-stable, no changes planned (status of 3 chronic medical conditions in place of 4 HPI)2) HTN-stable, no changes planned3) chronic afib-stable, no changes planned4) hypoxemia-new (Diagnosis-4 points for new problem, more workup planned)P) Discussed code status today. Patient wishes to be a DNR due to poor prognosis.(high risk for DNR discussion, order for DNR) Check CXR ( Data-1 point for radiology)
The history of 99226 compliant with four HPI and two ROS elements. The MDM is high complexity based on data and risk. The data has the required four points with one point for reviewing lab, two points for personally interpreting an EKG tracing and one point for discussing the CXR with the radiologist. In addition, the case is high risk based on IV opiate therapy, a high risk therapy based on the risk table guidelines.S) RLQ abdominal pain, sharp, started yesterday, constant (4 HPI)no CP, no SOB (2 ROS)O) Nothing neededHgb 13.6 (Data-1 point)EKG tracing personally reviewed- sinus rhythm without ST or TW changes (Data-2 points for personally reviewing tracing or image)Discussed CXR findings with the radiologist (Data-1 point for discussing test with performing physician)A) Patient on a PCA for back pain, no changes today (High risk for IV opiate management)P) Nothing else needed
I hope these common clinical examples offer further proof that documentation is key to staying compliant. Writing a novel is not required. As physicians, I think we tend to underestimate the level of complexity we encounter because we are used to it. We need to do a better job of documenting what we do and understand the rules we have been given to follow. Notice these notes are not long essays. They are strategically written to capture value in work we are doing but not currently describing in the correct manner. Don't be afraid to bill 99226 if the face-to-face encounter you provide is medically reasonable and necessary and your documentation supports CPT® 99226. In fact, if you think about it, patients in observation may not be "sick enough" to be admitted, but CMS has instructed us to use CPT® code 99226 for high complexity observation evaluations whose criteria is exactly the same as high complexity patients who are admitted as inpatients. Being observation does not mean they are too healthy for high complexity care. Always keep in mind documentation is key to getting paid, based on the rules we have been given, for the work we are providing.
DISTRIBUTION OF OBSERVATION SUBSEQUENT CARE CODES (99224-99226).
What is the distribution of CPT® code 99226 relative to other levels of service in this family of medical codes? The CPT® group 99224-99226 is pretty new. CMS has only recognized these codes since 2011. However, CMS has data explaining how often 99224, 99225 and 99226 have been used. The graphic below was obtained from the 2011 CMS Part B National Procedure Summary Files data (2011 zip file) showing how many CPT® 99226 encounters were billed and the dollar value of their services for Part B Medicare. As you can see in the image below, E/M code 99226 was billed 88,982 times in 2011 with allowed charges of $6,534,122.22 and payments of $5,153,258.29.

RVU VALUE
How much money does a CPT® 99226 pay in 2016? That depends on what part of the country you live in and what insurance company you are billing. E/M procedure codes, like all CPT® billing codes, are paid in relative value units (RVUs). This complex RVU discussion has been had elsewhere on The Happy Hospitalist. For raw RVU values, a CPT® 99226 is worth 2.96 total RVUs. The work RVU for 99226 is valued at 2.0. Make sure to review the complete list of RVU values on common hospitalist E/M codes. What is the Medicare reimbursement for CPT® code 99226? In my state, a CPT® 99226 pays just over under $100 in 2016. The dollar conversion factor for one RVU in 2014 is 35.8043.
My E/M reference card below has taught me that I should be billing for the work I'm providing and it has taught me how to document appropriately. You can see many more of my E/M lectures by clicking through on the provided link. If you need bedside help determining what level of care you have provided, I recommend reviewing the pocket card described below.
LINK TO E/M POCKET REFERENCE CARD POST
|

%20subsequent%20observation%20care%20code%20lecture.)
Tweet
Tidak ada komentar:
Posting Komentar