What does sequestration meant to physicians and hospitals? It means starting April 1st, 2013, The Centers For Medicare and Medicaid Services (CMS) will pay 2% less for Medicare services than they did on February 28th, 2013. Sequestration cuts are the result of a badly played political poker hand at the dysfunctional casino. On April 1st, 2013, will my post-sequestration medical opinion be worth 2% less than it was a month previously? Yes, it will.
For physicians and hospitals, the shot across the bow has been fired. What this cut says today is that no matter how perfect the game is played, politics will prevail. I've been a hospitalist now for ten years. In that decade of experience, I have seen many sticks and carrots implemented in various attempts to control healthcare costs and define quality. As I've said for the last five years on The Happy Hospitalist, the only way to control costs is to stop paying for it. It appears the sequestration has proved me right. If we simply stop paying for care, costs will decline.
Over my decade of experience, I have seen implementation of ORYX measures and SCIP requirements and never events that are, well, never mind. There are the MCCs and CCs and MS-DRG. There are the RAC audits and 30 day readmission penalties. There are the bundled care and accountable care programs. Plus, don't forget about the patient satisfaction penalties and a soon to be mortality penalty too. We've also got PQRS and E/M rules that turn honest physicians into criminals by default and despite all this noise, we still take care of patients. This original Happy Hospitalist ecard explains:
"I'm sorry ma'am, but Medicare will only pay me to cut out 98% of your tumor. If you want me to remove it all, I'll need to run your credit card for the difference."


But, no matter how well the rules are learned and how well the game is played, the house always wins. They control the money. If hospitals and doctors want to continue getting paid by the Medicare National Bank, they have to accept the consequences of their decision to play by the house's rules. It means 74 minutes of critical care and a total knee arthroplasty and a heart catheterization will all be worth 2% less on April 1st than they were on February 28th, 2013.
How private practices plan to absorb that cost is something only they can determine. Will they reduce their own costs? Will they delay capital expenditures? Will they reduce labor expenses by freezing wages or reducing benefits? Will they fire staff and place a greater burden of work on remaining employees? Will they increase health care deductibles or reduce 401K contributions for their employees? Will the doctors eat the costs and take home less pay?
Will practices attempt to increase revenue? Will they start charging patients for phone calls? Will they collect handicap parking application fees and charge for FMLA paperwork? Will they start collecting a 2% sequestration penalty fee? Will they charge for parking? Will they start selling vitamins and supplements in their office? Will they order unnecessary lab to boost ancillary services? Will they recommend unnecessary surgery to save their bottom line? Will they implement a concierge option and slowly but surely squeeze the Medicare patient out of their practice?
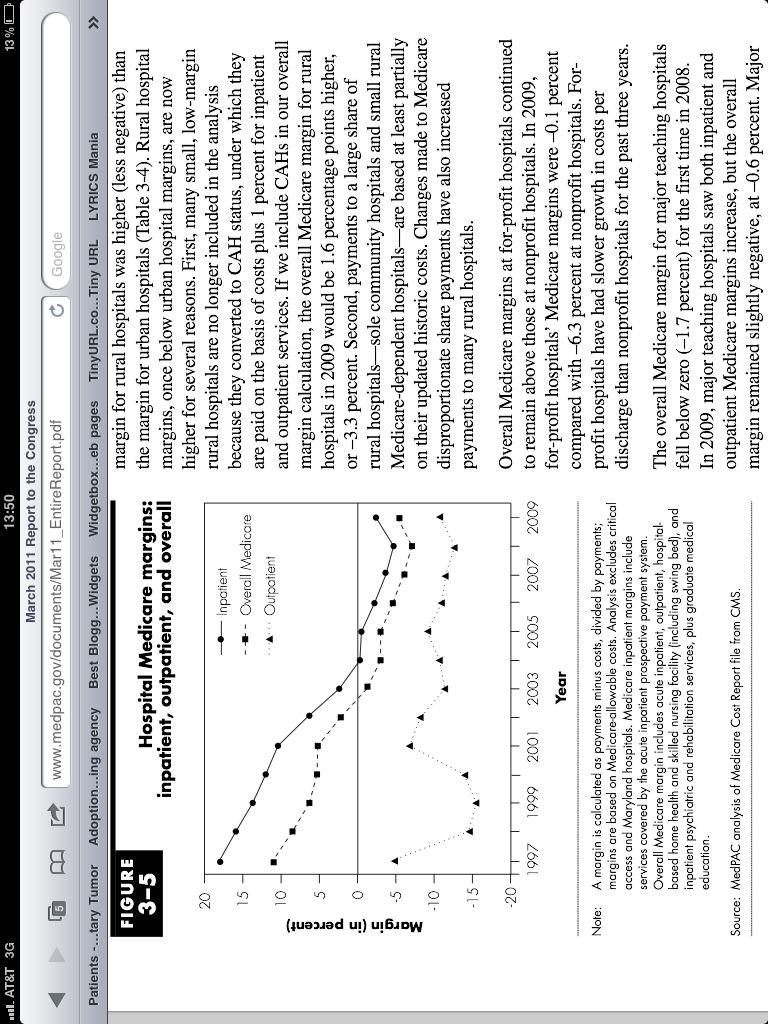
How will hospitals survive? Hospital profit margins have been negative for the better part of a decade. Billions of dollars have disappeared in an instant from operating budgets. How about all those hospital owned physician practices and all those teaching hospitals who need money to pay their residents? Who's going to eat that cost? The sequestration cuts are certain to wreak havoc on hospitals that can least afford the cut. Inner city systems will struggle and many hospitals may close.
What effect will sequestration have on hospitalists? That's hard to say. Much of our value comes from our ability to learn the system of sticks and carrots. We create efficiencies, reduce length of stay and play the revenue optimization games. Will compensation for hospitalists suffer under sequestration? That's hard to say. My gut instinct says no. We are still a growing field who's services are high in demand. The market is speaking loudly of the value we provide. If anything, I think sequestration places a continued demand and a rising premium for our service as a means of maintaining margins in this declining revenue scenario. In other words, our cost is the lesser of two evils.
The sequestration cuts should be a wake up call to all hospitals and physicians. Medicare and Medicaid are sinking ships without a captain. They are lost in a sea of debt with no dock to anchor at and the tough decisions that must be made are being ignored. Who's going to survive the Medicare axe? Those who are well prepared for life without their government cheese. If Washington can do it once, I guarantee they will do it again. Another day. Another poker hand. Another sequestration.
And now for a little sequestration humor with this original Happy medical ecard.
"Stop bitching about payment cuts at MY nursing station, doctor. If you're worried, sell your Mercedes and buy a Hyundai like the rest of us."
For physicians and hospitals, the shot across the bow has been fired. What this cut says today is that no matter how perfect the game is played, politics will prevail. I've been a hospitalist now for ten years. In that decade of experience, I have seen many sticks and carrots implemented in various attempts to control healthcare costs and define quality. As I've said for the last five years on The Happy Hospitalist, the only way to control costs is to stop paying for it. It appears the sequestration has proved me right. If we simply stop paying for care, costs will decline.
Over my decade of experience, I have seen implementation of ORYX measures and SCIP requirements and never events that are, well, never mind. There are the MCCs and CCs and MS-DRG. There are the RAC audits and 30 day readmission penalties. There are the bundled care and accountable care programs. Plus, don't forget about the patient satisfaction penalties and a soon to be mortality penalty too. We've also got PQRS and E/M rules that turn honest physicians into criminals by default and despite all this noise, we still take care of patients. This original Happy Hospitalist ecard explains:
"I'm sorry ma'am, but Medicare will only pay me to cut out 98% of your tumor. If you want me to remove it all, I'll need to run your credit card for the difference."

But, no matter how well the rules are learned and how well the game is played, the house always wins. They control the money. If hospitals and doctors want to continue getting paid by the Medicare National Bank, they have to accept the consequences of their decision to play by the house's rules. It means 74 minutes of critical care and a total knee arthroplasty and a heart catheterization will all be worth 2% less on April 1st than they were on February 28th, 2013.
How private practices plan to absorb that cost is something only they can determine. Will they reduce their own costs? Will they delay capital expenditures? Will they reduce labor expenses by freezing wages or reducing benefits? Will they fire staff and place a greater burden of work on remaining employees? Will they increase health care deductibles or reduce 401K contributions for their employees? Will the doctors eat the costs and take home less pay?
Will practices attempt to increase revenue? Will they start charging patients for phone calls? Will they collect handicap parking application fees and charge for FMLA paperwork? Will they start collecting a 2% sequestration penalty fee? Will they charge for parking? Will they start selling vitamins and supplements in their office? Will they order unnecessary lab to boost ancillary services? Will they recommend unnecessary surgery to save their bottom line? Will they implement a concierge option and slowly but surely squeeze the Medicare patient out of their practice?
How will hospitals survive? Hospital profit margins have been negative for the better part of a decade. Billions of dollars have disappeared in an instant from operating budgets. How about all those hospital owned physician practices and all those teaching hospitals who need money to pay their residents? Who's going to eat that cost? The sequestration cuts are certain to wreak havoc on hospitals that can least afford the cut. Inner city systems will struggle and many hospitals may close.
What effect will sequestration have on hospitalists? That's hard to say. Much of our value comes from our ability to learn the system of sticks and carrots. We create efficiencies, reduce length of stay and play the revenue optimization games. Will compensation for hospitalists suffer under sequestration? That's hard to say. My gut instinct says no. We are still a growing field who's services are high in demand. The market is speaking loudly of the value we provide. If anything, I think sequestration places a continued demand and a rising premium for our service as a means of maintaining margins in this declining revenue scenario. In other words, our cost is the lesser of two evils.
The sequestration cuts should be a wake up call to all hospitals and physicians. Medicare and Medicaid are sinking ships without a captain. They are lost in a sea of debt with no dock to anchor at and the tough decisions that must be made are being ignored. Who's going to survive the Medicare axe? Those who are well prepared for life without their government cheese. If Washington can do it once, I guarantee they will do it again. Another day. Another poker hand. Another sequestration.
And now for a little sequestration humor with this original Happy medical ecard.
"Stop bitching about payment cuts at MY nursing station, doctor. If you're worried, sell your Mercedes and buy a Hyundai like the rest of us."

More humor...
I just read a message from my hospital that says due to the across the board 2% sequestration Medicare payment cut that kicks in today, all employees are now expected to clock out when they use the restroom. They will be watching to ensure compliance. What a sad day to think it has come to this.
Tweet
Tidak ada komentar:
Posting Komentar